
Can Constipation Cause Back Pain?
Team Metabolic Health
Back pain is common and is usually caused by an injury or age-related degenerative conditions affecting the spine, spinal nerves, or muscles in the back. But injuries and age aren’t the only causes of back pain. Have you ever had back pain that seems unrelated to any injury? Surprisingly, this unexpected back pain may be a side effect of constipation.
Find out more about constipation-related back pain and what you can do about it.
What is constipation?
Almost everyone experiences constipation at some point in their life. The general medical definition for constipation is when you have three or fewer bowel movements a week, passing stool that’s dry and hard. But if your usual bowel movement schedule isn’t like others and is usually less frequent, true constipation is when there’s a change in your normal bowel movements.
Some people poop several times a day, while others poop only a few times a week. According to the American Society of Colon & Rectal Surgeons (ASCRS), individual constipation is pooping less often than normal or passing stool that’s rock hard and requires excessive straining. A slowdown in the movement of food waste through the digestive tract, or more specifically the colon, causes constipation.
Your digestive system absorbs as much nutrition as possible — carbs, protein, fat, vitamins, minerals, and other health-promoting nutrients — from the food you eat as it moves its way through. The food waste that reaches the colon is made up of nondigestible fibers and water.
A lot happens in the colon as the food waste moves through. The microorganisms that live in this part of your digestive tract feed off the fiber and make essential nutrients, the waste collects toxic substances for removal, and any remaining water is reabsorbed. The longer it takes for stools to move through the colon, the more water it removes, creating the dry, hard, and difficult-to-pass stool.
Constipation has many causes, including a change in diet, alterations in your usual routine, stress, or certain medications. For most people, constipation clears up on its own within a few days. However, if you continue to have infrequent or hard-to-pass poop for several weeks, you may have chronic constipation.
Symptoms of constipation
- Common constipation symptoms mostly center around your bowel movements and include:
- Having fewer than three bowel movements a week or changes to your normal bowel habits
- Passing rock-like pieces of stool (hard and small)
- Straining to pass stool
- Experiencing pain during bowel movements
- Lingering urge to poop after having a bowel movement
- More serious symptoms of constipation include:
- Inability to pass gas
- Bleeding during a bowel movement
- Blood in stool
- Constant stomach pain
- Not passing stool
- Vomiting
- Fever
On top of these symptoms, constipation may cause back pain, seeming completely unrelated to your tummy issues.
Can constipation cause back pain?
In a nutshell, constipation can cause back pain, especially in the lower back. The pain may occur because of a buildup of stool in the large intestines, leading to swelling that puts pressure on the spinal cord or spinal nerves.
Preliminary research also shows an association between constipation, an imbalance in the gut microbiome, and back pain. People who experience constipation are more likely to have an imbalance in bacteria in the gut and more severe lower back pain than people without constipation, according to a 2018 study published in Anesthesiology and Pain Medicine. The researchers theorize that the imbalance in the microbiome may affect communication between the gut and brain, influencing and exacerbating pain sensations. But this is preliminary evidence and more research is needed to better understand the connection between constipation, chronic back pain, and the microbiome.
Lower back pain is also a symptom of fecal impaction, a severe form of constipation that requires immediate medical attention. It’s a type of bowel obstruction where dry, hard stool gets stuck in the rectum, the last section of the large intestine that holds stool before elimination. Abdominal pain, bloating, and difficulty passing stool are other symptoms you may have with fecal impaction. Without immediate treatment, the impacted stool may tear through the intestinal wall, leading to an infection.
Conditions that cause both constipation and back pain
Constipation and back pain are symptoms that occur from any number of causes. Experiencing both symptoms at the same time can help pinpoint the underlying cause.
Constipation is one of many symptoms that affect people with irritable bowel syndrome (IBS), a functional gastrointestinal disorder where the gut and brain don’t work together as they should. Symptoms vary in type and severity with irritable bowel syndrome but may include abdominal pain, bloating, and changes in bowel habits.
Other conditions that can cause both constipation and back pain include:
If you have chronic pain, taking certain medications to manage your discomfort may cause or worsen constipation.
When to see a healthcare provider
If you have severe abdominal pain, difficulty passing stool, or signs of dehydration related to your constipation, seek immediate medical attention. You should also make an appointment with your doctor if you have severe constipation and back pain that lasts longer than a few weeks.
Severe back pain, numbness and tingling in the legs, difficulty controlling bowel movements (incontinence), or unexplained weight loss are also symptoms of concern that should benefit from a doctor’s evaluation.
Self-care for constipation and back relief
Making changes to your lifestyle may help you manage both your constipation and back pain. Increasing your fiber intake and managing stress may help relieve both symptoms. More fiber adds bulk to stool, making it easier to pass, reducing buildup and pressure. Stress may trigger IBS and exacerbate back pain and constipation.
Drinking plenty of water to stay hydrated can help prevent constipation. You also want to limit foods with little to no fiber, such as snack foods, fast food, and processed food.
Getting regular exercise also benefits constipation and back pain. Walking and yoga are good forms of physical activity that can improve bowel function and reduce symptoms of constipation. Exercise also releases the body’s natural painkillers to help reduce chronic back pain.
Your doctor may also recommend a stool softener and a bathroom routine that helps you find relief from constipation. Natural stool softeners like prunes, flaxseed, and psyllium may also help.
Final word
Constipation and lower back pain are common health complaints. Though back pain has many causes, you may not connect your chronic pain with your infrequent bowel movements, but constipation can cause lower back pain. Improving bowel regularity may help you get relief from your back pain, but you should talk to your doctor if your constipation persists.
FAQ
- What does constipation back pain feel like?
- Constipation back pain may cause a dull ache in the lower back. Over time, this may worsen and spread to the abdomen.
- How do I know if my back pain is bowel-related?
- Having a dull ache in your lower back and experiencing constipation at the same time may suggest that the two may be connected. Your doctor can truly determine if your back pain is bowel-related. They diagnose the cause of your pain based on symptoms and testing.
- Where is constipation pain located?
- Constipation pain usually affects the lower abdomen. You may feel pressure or bloating, but symptoms can vary.
Key takeaways:
- Constipation is when you have fewer bowel movements than usual or you strain to pass hard and dry stool.
- Constipation can cause back pain from pressure on the spinal cord or nerves due to a buildup of stool in the lower part of the large intestine.
- Constipation and back pain are symptoms with many causes and you should talk to your doctor when either symptom persists.
- Eating more fiber, drinking more water, and regular exercise can benefit both constipation and back pain.
Credit: healthnews.com
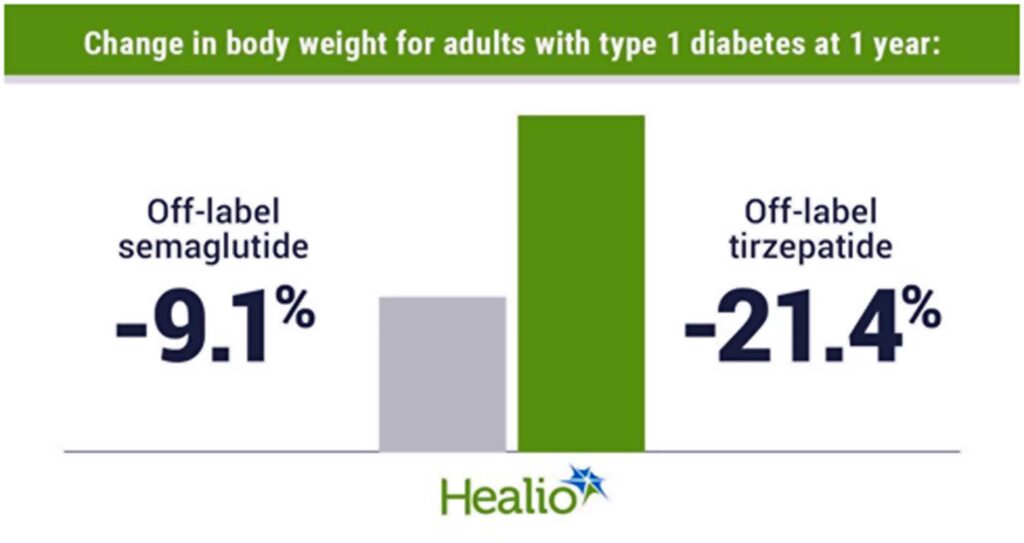
Off-label semaglutide, tirzepatide lower HbA1c and body weight in type 1 diabetes
Team Metabolic Health
Adults with type 1 diabetes had significant declines in body weight at 1 year of off-label semaglutide and tirzepatide use.
Use of both medications was associated with reductions in total daily insulin dose.
Adults with type 1 diabetes using either semaglutide or tirzepatide off-label had greater decreases in body weight and HbA1c than those not treated with either medication, according to a speaker.
As Healio previously reported, researchers at the Barbara Davis Center for Diabetes at University of Colorado Anschutz Medical Campus found adults with type 1 diabetes and overweight or obesity using tirzepatide (Mounjaro/Zepbound, Eli Lilly) off-label had a 0.67 percentage point reduction in HbA1c and an 18.5% decrease in body weight at 1 year. At the European Association for the Study of Diabetes annual meeting, University of Colorado researchers presented more data from their institution of adults with type 1 diabetes who used tirzepatide as well as semaglutide (Ozempic/Wegovy, Novo Nordisk) off-label.
Data were derived from Snell-Bergeon J, et al. OP 43. Presented at: European Association for the Study of Diabetes Annual Meeting; Sept. 9-13, 2024; Madrid.
“Off-label semaglutide and tirzepatide treatment resulted in significant weight loss and improved glycemic control in adults with type 1 diabetes, with no reported hospitalization for hypoglycemia or diabetic ketoacidosis,” Janet Snell-Bergeon, PhD, professor of pediatrics at the Barbara Davis Center for Diabetes at the University of Colorado Anschutz Medical Campus, said during the presentation.
Researchers conducted a retrospective chart review of 50 adults with type 1 diabetes and overweight or obesity who used semaglutide off-label and 50 adults who used tirzepatide off-label. Propensity score matching was used to compare data from semaglutide and tirzepatide users with 50 controls with type 1 diabetes and overweight or obesity who were not treated with either medication. Changes in BMI, body weight and HbA1c were assessed over a 1-year period.
Reductions in weight, HbA1c
Adults using tirzepatide had a 7.5 kg/m2 decline in BMI and semaglutide users a 3 kg/m2 decrease in BMI from baseline to 12 months (P for treatment difference < .0001). The tirzepatide group had a significantly greater reduction in BMI than controls starting at 3 months and continuing until the end of the study, whereas semaglutide users had a significantly greater decrease in BMI than controls beginning at 6 months and continuing through 1 year.
The tirzepatide group lost 21.4% of their body weight from baseline to 1 year and the semaglutide group achieved a 9.1% weight reduction in that same period (P for treatment difference < .0001). A weight loss of 10% or more at 1 year was achieved by 87% of adults using tirzepatide and 47% of those using semaglutide compared with no participants in the control group (P < .001).
Adults using semaglutide had a 0.54 percentage point decline in HbA1c at 1 year compared with a 0.68 percentage point decrease for those using tirzepatide. Both decreases were greater than the change in the placebo group (P = .008).
Change in total, basal and bolus insulin daily dose was significantly lower for adults using tirzepatide than those using semaglutide or controls. At 1 year, there was no significant difference in the change in total, basal or bolus insulin dose between the semaglutide and control groups.
“When we looked at total insulin dose per kilogram of body weight, there was a significant decrease [with tirzepatide], indicating that this went beyond just the loss of body weight and perhaps improved insulin sensitivity,” Snell-Bergeon said.
The change in BMI, body weight and HbA1c did not differ between adults receiving multiple daily insulin injections and those using an insulin pump. Snell-Bergeon said there was a trend toward greater HbA1c loss for adults receiving tirzepatide and using an insulin pump vs. semaglutide users or those using tirzepatide with multiple daily injections.
Dosing and safety
People using semaglutide began at a starting dose of 0.25 mg per week and were titrated up based on clinical guidelines. Of the group, 38 reached a maximum dose of 0.5 mg per week. For those using tirzepatide, the starting dose was 2.5 mg per week. Of the tirzepatide group, 16 reached a maximum dose of 5 mg, eight reached a maximum dose of 7.5 mg and 14 reached a maximum dose of 10 mg.
There were no reports of hospitalizations for DKA or hypoglycemia during the study. Three adults using semaglutide and one using tirzepatide discontinued the medication due to lack of response.
Snell-Bergeon said randomized controlled trials still need to be conducted to assess efficacy and safety outcomes for both medications among adults with type 1 diabetes.
Credit: healio.com
How Does Trulicity Work for Weight Loss?
Team Metabolic Health
Trulicity (dulaglutide) is FDA approved to treat Type 2 diabetes. It’s also approved to prevent heart problems in people with Type 2 diabetes and heart disease, or risk factors for heart disease.
Even though it can cause you to lose weight, Trulicity is not FDA approved for weight loss. Other medications similar to Trulicity that are FDA approved for weight loss include Wegovy (semaglutide), Saxenda (liraglutide), and Zepbound (tirzepatide).
Higher doses of Trulicity may cause more weight loss in people with Type 2 diabetes compared to lower doses.
Pix Credit: Getty Images
Living with diabetes comes with unique health challenges. Maintaining a healthy weight is one of them. Nearly 90% of U.S. adults with diabetes are considered overweight or obese. So naturally, many people with diabetes have questions about which diabetes medications can help you lose weight.
Trulicity (dulaglutide) is one potential option. It’s an FDA-approved medication for Type 2 diabetes when used along with a diabetes-friendly diet and exercise. And it’s also approved to lower the risk of heart problems in people with Type 2 diabetes and heart disease (or risk factors for heart disease). Although it’s not FDA approved specifically for weight loss, it can help in this arena as well. Here, we’ll discuss Trulicity and when it can be a tool for healthy weight loss.
How does Trulicity work for weight loss?
Trulicity is a glucagon-like peptide-1 (GLP-1) agonist. It stimulates insulin release when you eat to help control your blood glucose (sugar) levels. Trulicity isn’t FDA approved for weight loss specifically. But weight loss may be an added benefit of taking Trulicity.
GLP-1 is a type of incretin hormone. Incretins are released naturally in the body after you eat. They stimulate insulin release from your pancreas (an organ behind your stomach). This prevents blood glucose levels from rising too high.
Trulicity also slows down how quickly food travels from your stomach to your intestines. This helps you feel full sooner after eating, making you eat less. This effect helps regulate blood glucose and it can also lead to weight loss.
What does the research show about Trulicity and weight loss?
Trulicity is one of several diabetes medications that can cause weight loss. The amount of weight loss you’ll lose depends on several factors, including your Trulicity dose, how long you take it, and your starting body mass index (BMI). Generally, people tend to lose more weight with higher doses, especially if they have a higher body weight initially.
Comparing GLP-1 agonists. Several GLP-1 agonists are on the market today, and they have differences to consider.
Ozempic vs. Trulicity. Compare two common GLP-1 agonists used to treat Type 2 diabetes.
Comparing weight loss medications. Several medications are FDA-approved for weight loss, and many more are on the horizon.
In 2020, a large randomized controlled trial (the best type of study to look for cause and effect) was conducted to see how different Trulicity doses stacked up against each other. In the study, over 1,800 participants already taking metformin for Type 2 diabetes were started on Trulicity. Metformin is a common first-choice option for treating diabetes.
This study found that the amount of weight people lost, and how much their blood glucose decreased, was dose-related. People taking Trulicity 4.5 mg lost more weight (about 10 lbs) than people taking Trulicity 3 mg (about 9 pounds) or 1.5 mg (about 7 lbs) after about 9 months of treatment. Higher doses of Trulicity also decreased blood glucose more than lower doses.
The medication can be injected subcutaneously (underneath the skin) in the upper arm, thigh, or abdomen (belly). You’ll only need to inject Trulicity once a week. Be sure to use a different injection site each week. This prevents lumps from forming underneath your skin.
What’s a typical Trulicity dosage?
The starting dose of Trulicity is typically 0.75 mg once a week. You can inject Trulicity at any time of day, without regard to meals. So, pick a day and time that’s convenient for you. Just make sure you inject your dose on the same day each week.
After 4 weeks, your dose may be increased to 1.5 mg if your blood glucose is still high. Then, if your blood glucose remains high after 4 weeks, your dose may be increased by 1.5 mg every 4 weeks until your blood glucose levels are controlled. The maximum dose is 4.5 mg once a week.
Keep in mind that blood glucose goals may vary from one person to the next. So talk to your diabetes care team about what your target blood glucose range is before starting Trulicity or other diabetes medications.
Trulicity side effects
The most common Trulicity side effects are gastrointestinal (GI) side effects. People most commonly experience GI side effects within the first few weeks of starting Trulicity, such as nausea, vomiting, and diarrhea. A decreased appetite, stomach pain, and indigestion can also occur.
Less common but more serious side effects include gallbladder disease and kidney damage. In rare cases, people taking Trulicity have reported pancreatitis. And thyroid tumors have been seen in animal studies, but haven’t been confirmed in human studies.
Low blood glucose (hypoglycemia) can also occur. But it’s less common with Trulicity than some other diabetes medications, such as insulin. Hypoglycemia is typically defined as blood glucose less than 70 mg/dL. Some common signs of hypoglycemia include:
- Shakiness
- Faster heart rate
- Sweating
- Hunger
- Anxiety
- Sleepiness
- Feeling weak
- Tingling
- Confusion
- Dizziness
Check your blood glucose right away if you experience any of these symptoms. Follow instructions from your diabetes care team for how to treat hypoglycemia (such as the “15-15 Rule”), and notify them as soon as possible.
Are GI side effects worse with higher doses of Trulicity?
Not usually. You may experience GI side effects with any dose of Trulicity. But most people don’t experience worsening GI side effects as their doses are increased. In fact, side effects are most likely when you first start taking Trulicity. Severe side effects are uncommon at any dose.
Comparing GLP-1 agonists, such as Ozempic vs. Trulicity
Ozempic (semaglutide) and Trulicity are both GLP-1 agonists. They’re both injectable medications, and they’re both FDA approved to treat Type 2 diabetes and lower the risk of heart attack, stroke, and death in people with Type 2 diabetes and heart disease. What’s more, neither medication is FDA approved for weight loss, though they can both cause weight loss when used. However, two other GLP-1 agonists are FDA approved for weight loss:
Wegovy (semaglutide)
Saxenda (liraglutide)
Additionally, Zepbound (tirzepatide) is another medication that’s closely related to GLP-1 agonists and FDA approved for weight loss.
There are no studies directly comparing Trulicity to the GLP-1 inhibitors that are FDA approved for weight loss. But research has shown that Wegovy is more effective for weight loss than Saxenda. And Zepbound may cause even more weight loss than Wegovy. If you’re interested in trying any of these medications for weight loss, talk to a healthcare professional about the risks and benefits of these medications.
Good to know: The active ingredient in Ozempic (semaglutide) is also available as Rybelsus, and the main ingredient in Saxenda (liraglutide) is also available as Victoza. Tirzepatide (the ingredient in Zepbound) is also available as Mounjaro. Rybelsus, Victoza, and Mounjaro are only FDA approved for Type 2 diabetes. They’re not currently FDA approved for weight loss.
How long does it take Trulicity to work for weight loss?
How long it takes to work depends on personal factors and the Trulicity dose you’re using. The amount of weight people lose with Trulicity can vary for several reasons, including their diet and exercise routine as well as their starting weight before treatment.
In clinical studies, people taking Trulicity 4.5 mg lost about 6 lbs to 7 lbs about 3 months after starting it. By about 9 months, they’d lost about 10 pounds. Although people taking Trulicity 3 mg and Trulicity 1.5 mg doses also lost weight, they didn’t lose as much.
The bottom line
Trulicity (dulaglutide) is a glucagon-like peptide-1 (GLP-1) agonist that treats Type 2 diabetes when combined with diet and exercise. It can also be used to prevent heart problems in people with Type 2 diabetes and existing heart disease, or risk factors for heart disease.
While Trulicity isn’t FDA approved for weight loss, it’s been shown to help people lose weight, especially at higher doses (4.5 mg per week). The most common side effects are gastrointestinal-related, like nausea, vomiting, and diarrhea.
Trulicity isn’t recommended in people without Type 2 diabetes. Other GLP-1 agonists, like Wegovy (semaglutide) and Saxenda (liraglutide), are FDA approved for weight loss specifically. So is another medication that’s closely related to GLP-1 agonists called Zepbound (tirzepatide). Talk to a healthcare professional if you’re interested in trying a GLP-1 agonist for weight loss.
Credit: goodrx.com
Six common flying with food allergies myths
Team Metabolic Health
A recent review in Archives of Disease in Childhood presents common misconceptions regarding food allergies during air travel and discusses strategies to help prevent them.
Background
Food-allergic passengers feel heightened anxiety while flying due to the perceived risk of peanut or tree nut particle exposure through airplane ventilation systems. Food allergies can result in anaphylaxis, a life-threatening allergic response. Fear of severe responses lowers quality of life, particularly during holidays and travel. Dispelling myths about air travel-related food allergies could increase confidence among food-allergic individuals.
About the review
The present review discusses myths and evidence regarding in-flight food allergies and mitigation strategies based on the 2023 United Kingdom Civil Aviation Authority (CAA) report.
Common myths and evidence regarding food allergies during air travel
Myth 1: Allergic responses are more frequent on airplanes
The evidence: Research shows that individuals with food allergies are 10 to 100 times less likely to develop allergic reactions on a flight. The low frequency of allergies among food-allergic passengers may be attributed to the measures taken when flying.
Myth 2: Aerosolized food allergens are a major concern
The evidence: Allergies to aerosolized meals are infrequent, except for exposure to vapors from fish or seafood or occupational allergens such as wheat flour in baker’s asthma and seafood in fish market workers.
Myth 3: Peanut particles in ventilation systems trigger reactions
The evidence: Individuals with food allergies think peanut particles may transfer through aircraft passenger cabin ventilation systems and induce allergic responses. However, such occurrences are rare. Deshelling roasted peanuts can produce low-level but detectable peanut allergens in the air. However, aircraft ventilation systems successfully remove most nut particles in circulation. Allergies most likely result from the unintentional eating of allergen-containing food and the spread of allergen residues from seat or tray surfaces to hands, subsequently transferred to safe food ingested.
Myth 4: Nut consumption bans prevent in-flight allergies
The evidence: People think requesting passengers not to consume nuts can prevent in-flight nut allergies. However, peanut residues on seats from prior flights cause significantly more exposure than nut-eating on a current flight. Cleaning seat surfaces, tray tables, and seat-fixed entertainment systems with wet wipes before beginning flight travel is far more effective in reducing allergy risk. Nut ‘bans’ might sometimes lead to false reassurance.
Myth 5: Homemade food is safer than airline meals
The evidence: Individuals with food allergies frequently avoid airline meals and carry homemade food. However, food allergies on a flight occur after consuming homemade food and items purchased on flights, typically due to human errors in buying items that may contain allergens. Airlines frequently provide allergen-free meals if informed in advance.
Myth 6: Medical authorization is required to carry adrenaline injectors
The evidence: Individuals assume medical authorization is necessary to transport adrenaline injectors on an airplane. However, UK legislation permits individuals prescribed adrenaline autoinjectors to carry them without such restrictions.
Onboard medical tool kits rarely include autoinjectors, and cabin crew members may not always have permission to use autoinjectors. Thus, food-allergic passengers with anaphylaxis risk should carry two adrenaline injectors in cabin baggage with them when flying.
Air circulation systems for passenger cabins on commercial planes
Environmental control systems (ECS) in airplanes regulate cabin air pressure, supply, and temperature to provide passengers and cabin crew with a pleasant atmosphere. The systems assure the removal of carbon dioxide, smells, and other airborne impurities, necessitating high airflow rates throughout the cabin. Air enters the cabin from overhead distribution outlets in a regulated circular airflow pattern. The pattern causes air to circulate throughout the aircraft, limiting the spread of pollutants.
ECS delivers approximately 20 cubic feet of air per minute per passenger, resulting in a full cabin air exchange every three to four minutes. In commercial airplanes, over 50% of the air intake is recirculated air passed through high-efficiency particulate air (HEPA) filters. HEPA filters remove 99.97% of particles at 0.3 µm, including dust, vapors, and microbiological diseases. They also capture the majority of aerosolized food particles. HEPA filtration and the frequency of full cabin air exchange (15-20 times per hour) lower peanut residue in dust suspended in cabin air.
Conclusions
Based on the findings, peanut and tree nut allergies are not disseminated via airline cabin ventilation arrangements but through accidental dietary ingestion of allergens or their residues on seat surfaces.
Announcements recommending that passengers avoid nuts may not prevent in-flight responses. Cleaning sitting places with a moist wipe is an excellent method.
Airlines must have defined food allergy-related policies mentioned on their websites and routinely followed by cabin crew and ground workers.
‘Buffer zones’ in which passengers surrounding a food-allergic traveler are urged not to consume the allergen may give reassurance but pose concerns about which allergens other passengers can be asked not to ingest.
Credit: news-medical.net
Food packaging should have labels on front about health impact, says WHO
Team Metabolic Health
Packaged food and drinks should have easy-to-read nutritional information on the front of the products to help consumers make healthier choices, according to the first-ever World Health Organization draft guidelines that stopped short of recommending harsher warning labels.
Increased consumption of processed foods high in salt, sugar and fat is a key driver of a global obesity crisis, with more than a billion people living with the condition and an estimated eight million early deaths every year due to associated health problems like diabetes and heart disease, WHO data shows.

A customer shops for dairy products at a grocery store in Saint Petersburg, Russia. REUTERS/Anton Vaganov/File Photo
Yet governments have struggled to introduce policies to curb the epidemic. Currently, only 43 WHO member states have any kind of front-of-package labelling either mandatory or voluntary, the UN agency told Reuters, despite evidence showing labels can affect buying behaviour. The WHO began work on the draft guidelines, which have not been previously reported, in 2019. They aim “to support consumers in making healthier food-related decisions,” Katrin Engelhardt, a scientist in the Nutrition and Food Safety department of the WHO, told Reuters by email.
A public consultation on the guidelines closed on Oct. 11 and the finalized version will be released in early 2025.
The WHO’s guidance recommends governments implement “interpretive” labels that include nutritional information and some explanation of what that means about the healthiness of a product.
An example would be NutriScore, developed in France and used in a number of European countries, which ranks food from A (green, containing essential nutrients) to E (red, containing high levels of added salts, sugars, fats or calories).
Chile and several other countries in Latin America use a tougher system, with warnings that a food is “high in sugar”, salt or fat on the front of the package, in a black octagon that resembles a stop sign. Food labelling expert Lindsey Smith Taillie, co-director of the Global Food Research Program at the University of Chapel Hill, North Carolina, said the food industry has pushed back against warnings and favours “non-interpretive” labels, which include the nutrient information but no guide on how to understand what that means, such as those used in the United States. This week, U.S. Senator Bernie Sanders announced plans for a Senate hearing on tougher food labelling in December. While the WHO recommendation goes a step further than the industry’s preference, it “is fairly weak,” Taillie said.
Credit: Reuters
Could Weight-Loss Drugs Help Get People Back to Work?
Team Metabolic Health
The British government announced a multimillion dollar pharmaceutical partnership with Eli Lilly, including a trial that will study the impact of a weight-loss drug on work and productivity.
Around one in four adults in Britain is obese, according to estimates from the country’s National Health Service, and the problem costs the public health care system billions every year.
Now, the government says that weight-loss injections might be part of the solution, and might even help boost Britain’s productivity, which has been sluggish for years.
Studies show that people with obesity are more likely to find that ill health affects their productivity and attendance at work. On Monday, the government announced a 279 million pound (around $365 million) investment from the pharmaceutical company Eli Lilly. Among other things, the investment will help explore new ways of delivering health services to people living with obesity, and include a five-year trial of the company’s drug tirzepatide, also known as Mounjaro, which is used to treat diabetes and for weight loss.

On Monday, the British government announced a five-year trial of the weight-loss drug tirzepatide, also known as Mounjaro. Credit: George Frey/Reuters
The trial, in the Greater Manchester area in northern England, will study the effectiveness of tirzepatide in bringing about weight loss, preventing diabetes and tackling obesity-related health conditions. It will also aim to collect data on whether the drug leads to changes in participants’ employment status and sick days from work, according to a statement from the Health Innovation Network, the innovation arm of the N.H.S.
The government said that up to 3,000 people could eventually take part in the study.
Prime Minister Keir Starmer, speaking to BBC Breakfast on Tuesday, said he believed the drugs could be “very important for our economy and for health,” adding that tirzepatide “will be very helpful to people who want to lose weight, need to lose weight, very important for the economy so people can get back into work.”
Wes Streeting, Britain’s health secretary, wrote in an opinion piece in The Telegraph that the country’s “widening waistbands are also placing significant burden on our health service,” noting that illnesses linked to obesity cost the country’s health service roughly $14 billion a year.
“The long-term benefits of these drugs could be monumental in our approach to tackling obesity,” Mr. Streeting wrote. “For many people, these weight-loss jabs will be life-changing, help them get back to work and ease the demands on our N.H.S.”
But he added that “there must remain a responsibility on us all to take healthy living more seriously,” and said that the country’s health service “can’t be expected to always pick up the tab.”
Credit: The New York Times
The dark reality of melatonin behind India’s USD289 million wild chase for good sleep
Team Metabolic Health
Synopsis
Most Indians are sleep-deprived and are turning to melatonin for a better night’s rest. The global melatonin market reached USD2.15 billion in 2022, and India’s sleep aid market is projected to generate USD289 million in revenue in 2024 alone. While melatonin is often considered harmless, everything has a flipside.
We all know about ‘city that never sleeps’. Now, move over to a ‘world that never rests’. You are exhausted but can’t sleep. What do you call that feeling? According to Juhi Bajaj, a 21-year-old home tutor and devout follower of Instagram sleep coach Cayla Solomon, it’s simply “brain-fried”. Ironically, Bajaj’s WhatsApp status reads “sleeping”, though she hasn’t had a good night’s rest in months – until she caved to the trend sweeping the sleep industry: melatonin supplements.
With a purple bottle of Vicks ZZZquil gummies on her side table, Bajaj is far from alone in this quest for better sleep. The melatonin supplement market, valued at USD2.15 billion in 2022, is booming. But why is everyone suddenly so obsessed with catching ZZZs?
Blame the urban grind where time is all – ‘cruel, a thief, and a villain’. It sends people on a wild chase round the clock, trading their precious sleep for all their unfulfilled dreams.
To reclaim their forty winks, many are turning to melatonin. Once naturally produced by the body, it’s now bottled for convenience, promising to nudge sleep cycles back on track.
But is it the solution we need? Here’s what the numbers say.
In 2023, global melatonin production hit 3,500 thousand tonne. It is projected to skyrocket 134% to 8,200 thousand tonne by 2034.
And the world is wide awake, waiting for more. This is their story.
Munching on melatonin
Indians are waking up to melatonin in a big way. The market is estimated to grow at a strong CAGR of 10.4% from 2023 to 2033. In 2024 alone, India’s sleep aids market is expected to generate a solid USD289 million in revenue. And with the overall sleep industry valued at INR12,000 crore-INR14,000 crore, the demand is clearly rising.
So, what’s the top choice for sleep aids? Anything but a tablet.
Avnish Chhabria, founder of Wellbeing Nutrition, told ET Prime that global brands are already eyeing India’s growing appetite for supplements, including melatonin. Australia’s Swisse, for example, launched its SwisseMe Melatonin Gummies in India in 2022, and has quickly caught on.
But Indian brands like Wellbeing Nutrition aren’t backing down. Their plant-based melatonin sleep melts (available in 5mg or 10mg) are designed to promote relaxation and better sleep.
What’s their recipe? Chhabria explains the company’s ‘Oral Thin Strip’ technology allows melatonin to be delivered directly through the buccal layer of the mouth, ensuring 100% absorption into the bloodstream bypassing the gut.
When it comes to sales, quick-commerce platforms like Blinkit and Zepto are Chhabria’s go-to picks. With the company’s ARR (annual recurring revenue) surging from INR100 crore to a projected INR240 crore this year, it is evident that sleep-deprived Indians are driving this growth.
An e-mail sent to P&G, the leader in the segment with Vicks commanding 60% of the market share, remained unanswered until the time of publishing this article.
Manju Sharma, a 58-year-old homemaker in Delhi’s Sarita Vihar and single parent to a software engineer working odd hours, has found solace in a melatonin spray to catch some sleep between her son’s US-timed shifts. “It’s been three months since I started using melatonin spray [Carbamide Forte Melatonin 5mg]. Just two-three sprays and I am asleep in 15-20 minutes,” she shares.
But does it guarantee a morning as fresh as a daisy? Not quite.
The dark side
While the spray initially helped Sharma achieve restful sleep, she gradually began to feel heavy-headed upon waking up. Does she blame the product? Of course not. “Perhaps it is the milkman buzzing the doorbell or the barking dogs,” she muses.
Meanwhile, an ENT clinic, just a few blocks away, reported a case of acute shortness of breath in a patient who combined her bronchodilator with the melatonin spray. The patient, a young lawyer, was promptly transferred to the nearby Apollo Hospital where her condition improved, suggesting that these sprays may not be suitable for individuals with lung diseases – at least in some cases.
Does research back this up?
The European Medical Journal has found evidence indicating that melatonin use can exacerbate night-time asthma symptoms by constricting airways. This is due to its activation of the melatonin MT2 receptor, which influences the circadian rhythm and can counteract the effects of bronchodilators, particularly at high dosages.
So, is a moderate amount safe for long-term use?
Neurologists say no.
Here’s why.
As we age, our body’s melatonin levels naturally drop, which can lead to poor sleep quality or even insomnia. While melatonin supplements are widely available and popular for treating sleep issues, they are not a long-term solution. “Melatonin is most effective for temporary problems like jet lag or shift work disorder,” explains Praveen Gupta, principal director and head of neurology at Fortis Hospital, Gurugram. Taking it without a proper diagnosis won’t address the underlying sleep disorder.
The challenge also lies in figuring out the right dosage. With so many forms – patches, sprays, gummies, syrups, melts – each featuring different absorption rates, self-dosing can get a bit tricky. Unregulated use can cause side effects like dizziness, headaches, nightmares, palpitations, and even brain fog.
Without medical supervision, overdosing is a real risk. Take 27-year-old Niharika Basu, a BPO employee in Gurugram. Struggling with sleep due to irregular work hours, she tried melatonin gummies on a friend’s recommendation. Assuming more would be better, she took two 5mg gummies – unaware the typical starting dosage is just 1mg-3mg. A few hours later, she felt drowsy, disoriented, and nauseous – symptoms indicative of an overdose.
For those with conditions like epilepsy or heart issues, melatonin can be especially risky. “Melatonin can be helpful,” says Delhi-based nutritionist Divya Gandhi, “but overuse can lead to toxicity, and long-term use may disrupt neurotransmitters, triggering anxiety and worsening sleep once stopped.”
It is important to remember that, even though it is non-habit forming, melatonin is still a drug that should be used judiciously,” Gandhi adds.
Despite its availability over the counter (OTC) in India, melatonin is tightly regulated in countries like the UK, the EU, Japan, and Australia, where it is available only by prescription.
Doctors in India express concerns about dosages as high as 20mg being available OTC, warning that it should be used cautiously.
No child’s play
Sure, the adage goes, ‘Every child you encounter is a divine appointment’ but in no way does it imply parents can surrogate for a pediatrician and meet those appointments.
If the child is having trouble sleeping or is too active during the night, the young millennial parents are self-administering melatonin gummies to their children – regardless of whether it’s suitable for their age-group.
“The easy access to melatonin gummies can lead to self-medication, skipping proper diagnosis, and exposing children to unknown risks,” warns Gupta. Prolonged use, especially in young children, could stall brain development, leaving their minds dull.
In some cases, long-term melatonin use in children has been linked to delayed puberty, though this remains debated.
“Children naturally produce enough melatonin. Giving them supplements can cause dependency and lead to harmful effects,” cautions Gandhi. “Unfortunately, many parents turn to Google and Instagram for health advice instead of consulting professionals. It’s worrying.”
But does this stop parents? Not really.
On X (formerly Twitter), countless parents rave about the effects of melatonin on their kids, especially the US version of Vicks PURE Zzzs Kidz Melatonin Gummies. Amazon reviews hail it as a trusted household product.
A 2022 study highlighted the surge of 150% in melatonin sales between 2016 and 2020, leading to increased access among children.
As a result of this, in the US, from 2019 to 2022, Center for Disease Control and Prevention (CDC) reported 11,000 emergency department visits due to unsupervised melatonin ingestion by children aged five and under, often involving flavoured products.
If that’s not enough to raise an alarm, the US poison-control centre reports about melatonin ingestion by individuals aged 19 and under rose from 8,337 in 2012 to 52,563 in 2021, with hospitalisations and serious outcomes also increasing, particularly among teenagers and children aged 5 and below.
Though India lacks kid-specific melatonin supplements, parents aren’t hesitating to let their children take a bite of their gummies or use a sleep melt.
“They would be better off with fresh cherries, soaked walnuts, or bananas,” Gandhi suggests, noting that these foods can naturally boost the body’s melatonin production.
It’s all psychological
A Delhi-based clinical psychologist revealed to ET Prime that the long-term use of supplements can be traced back to classical conditioning. Users often develop habitual behaviour, regardless of whether the product has potential for physiological dependence.
This behaviour is fuelled by psychological trust and reliance on the supplement, creating a placebo-like effect where users feel the supplement is essential for their well-being.
This creates a psychological dependence, where the perceived need for the supplement becomes deeply entrenched in daily routines, making it tough to quit without feeling anxious or distressed. Moreover, the ritualistic aspect of taking supplements can offer a sense of control and security, further strengthening the behaviour.
And when you do try to stop, withdrawal symptoms may follow.
One user, who turned to melatonin gummies for exhaustion and anxiety-induced insomnia, described her withdrawal: “What promised to be a sleep solution quickly turned into a headache – literally.” She faced persistent headaches, mood swings, and anxiety that disrupted her daily life for days.
This could be partly psychological, but it might also be the body’s physiological rebound after discontinuing prolonged melatonin use.
“Even harmless things, when overused or abused, can become harmful,” says Gupta.
The jury is still out
In India, a study conducted back in 2015 found that 93% of Indians are sleep-deprived, and 34% have sleep apnea. We have surely come a long way, but here’s a quick reminder before we call it a wrap – Melatonin supplements do work – but on all? The same way? Nay-nay.
As we took leave of Bajaj, the home tutor cited earlier, her phone buzzed with a new Instagram notification from Solomon, her favourite sleep coach. But this wasn’t just any notification – it was a reminder for her melatonin gummy, a signal that sleep in the modern world is as much about routine as it is about rest.
Because eventually, for many, it’s not just about finding sleep – it’s about managing it.
And so, the cycle continues.
(Graphics by Sadhana Saxena)
Credit: ET World
The great pharmaceutical-academic merger
Team Metabolic Health
As drug companies fret over their finances, they are increasingly partnering with universities to help with early-stage research
Pharmaceutical companies are often lambasted for rising drug costs. For example, the price of new drugs entering the US market in 2023 was 35% higher than in 2022. According to an analysis from Reuters, part of the increase is due to a move to develop therapies for rare diseases: because fewer people have those condition, drugmakers push up the per-dose price to recover their costs. But the cost of developing drugs for more common diseases, including cancers, is also rising rapidly.
In 2019, pharmaceutical companies spent $83 billion dollars on research and development. After accounting for inflation, that’s roughly 10 times what the industry spent in the 1980s, according to the US Congressional Budget Office. A 2024 study showed that the share of sales revenue devoted to research spending rose from 12% in 2008 to 18% in 2019, and drugmakers are beginning to feel the pinch.
In addition to rising research costs, several blockbuster drugs will soon be old enough to be reclassified as generic, meaning their developers are set to lose their status as the exclusive manufacturer, says Magid Abou-Gharbia, founding director of the Moulder Center for Drug Discovery Research at Temple University. “When that happens, you can kiss the money goodbye,” he says.
Drug companies are increasingly looking to academics in a bid to mitigate some of these financial burdens. This often involves university researchers doing early-stage drug discovery before pharmaceutical companies take over to push a novel compound through clinical trials and get it to market. “This trend is not entirely new,” says Karl-Heinz Altmann, a synthetic organic and medicinal chemist at the Swiss Federal Institute of Technology (ETH), Zurich. “But it does have momentum now.”
Financial booster
In the life sciences, corporations have been scaling back their in-house research since the 1980s. According to the Nature Index, which tracks the output of 82 scientific journals, research partnerships between companies and academic institutions more than doubled between 2012 and 2016.
A 2022 report from the Association of the British Pharmaceutical Industry found 2,687 links between the UK pharmaceutical industry and academia in 2022, compared with 1,134 in 2003. In other words, collaborative work with academics is making up a larger share of research by private companies, including drugmakers.
“Pharmaceutical companies are moving to work more with academic centers to reduce their risk exposure,” says Kelly Chibale, an organic chemist and director at the University of Cape Town Drug Discovery and Development Centre. “It’s not a coincidence that Boston in the US or Oxford and Cambridge in the UK have so many major pharmaceutical companies. They’re based there because that’s where the academics that they want to collaborate with are.”
From pharma’s perspective, the proof-of-concept stages of drug development are laden with the risk of failure—something their accountants are keen to avoid. By comparison, academia is relatively unbothered by failure if lessons can be learned and—crucially—if papers can still be published. But even with spinout and start-up companies, universities lack the infrastructure to progress a novel compound much further than proof of concept. Clinical trials are just too expensive. If done right, collaborations between the two worlds can be mutually beneficial.
Along with the shift of drug discovery to the academic world, larger numbers of researchers are moving from pharmaceutical companies into academic roles.
For instance, Altman worked at Novartis until 2003, when he moved to ETH Zurich. “I was offered the job. I didn’t seek it out,” he recalls. “It was a difficult decision to go from a well-established environment where you know people to a situation where you have to start from scratch. It’s not like you’re a professor moving from one university to another where you can take your research with you. What I did at Novartis stayed there. All I had was a lab and a budget to develop ideas.”
The move involved a number of serious considerations—starting with the drop in salary. “I don’t think anything that a head of research can earn in industry would ever be matched by a university,” Altman says. “I would probably make twice as much money if I’d stayed in industry.” But he says the freedom to choose a research path was worth the sacrifice in salary.
Altman’s move into academe is part of a wider trend within drug development research as more people move back and forth between industry and universities. “Industry is stepping out of the very early stages because it’s becoming more and more expensive,” says Peter Nussbaumer, managing director at the Lead Discovery Center in Dortmund, Germany, a translational drug research company founded by the Max Planck Society’s technology transfer arm, which collaborates with academic partners.
As more early-stage research moves from industry to academia, so too do people, Nussbaumer says. And academic drug discovery centers have become a destination for them.
Those who dare, win
In 2008, Abou-Gharbia left his job as a senior vice president at Wyeth Research—which was later acquired by Pfizer—to become a professor of pharmaceutical sciences at Temple University. As part of his recruitment, Abou-Gharbia was tasked with kick-starting drug discovery research there. The concept was something of a novelty at the time, he recalls. “There were only a few drug discovery centers in universities,” he says. Now, according to a 2017 study authored by Abou-Gharbia, there are close to 100 such centers in the US alone.
A growing trend
A year after starting at Temple, Abou-Gharbia was awarded a $1 million stimulus grant from the National Institutes of Health. He then wrote a pitch to establish a drug discovery center, which would include cutting-edge technologies used by the pharmaceutical industry. The university’s leadership approved the proposal and backed it with about $8.2 million, which allowed the center to recruit researchers and build laboratories.
The Moulder Center is celebrating its 15th anniversary this year. Since its founding, the center has received more than $35 million in outside support—enough to enable its staff to publish more than 180 papers in peer-reviewed journals and file more than 30 patents. Moulder has also created four spin-off companies and trained many future researchers in modern drug discovery and development. “Many universities ask me how to establish similar centers and I tell them you need university support and money,” Abou-Gharbia says.
You also need industry researchers to be readily accepted into academic roles, as Abou-Gharbia was. Such a career move used to be hard to pull off. Though being poached by industry was a well-trodden path for academics, going in the other direction was relatively rare until just a couple of decades ago. This is still the case in much of the EU, according to Nussbaumer. “It’s much easier to go back and forth in the UK and US,” he says. “Not so much in mainland Europe.”
Altman agrees but says Germany and other EU countries are beginning to catch up. “It’s starting to become a bit more relaxed,” he says.
Universities used to be rigid and highly particular about what kind of experience qualified a person for the job, Nussbaumer says. And there was a question of values: Are you in it for the money or the science? But those boundaries have become less defined in recent years, thanks in part to the promise that researchers can achieve scientific progress and make money by building small companies on the back of their research with the hope of attracting the interest of a larger drug developer.
Fernando Albericio, an organic chemist at the University of KwaZulu-Natal, has noticed that this way of thinking has also started to inform the career goals of students and young researchers. “In the past, a PhD student typically wanted to work in academia for life,” he says. These days, their ambition more often is to start a company.
“The number of spin-off companies is rising rapidly, and they have a sense of being the bridge between academia and pharmaceutical companies,” Albericio says. Drug discovery centers and spinouts enable the academic scientist to carry on their work with one foot in each door.
Drugmakers’ courtship of academic scientists is about more than quelling their financial fears. “It’s part of it, sure. But it’s also that drug discovery has gotten harder because the easier drugs to discover have already been discovered,” says preclinical pharmacologist Charles Hart, who earlier this year became codirector of the Small Molecule Discovery Center at the University of California, San Francisco (UCSF), after 30 years in biotech. “We need new drugs in cancers and new diseases like COVID-19 and other infectious agents, which is just really hard.” Hart says that industry also wants and needs access to the cutting-edge know-how that academic researchers possess.
University-based drug discovery centers and their start-up firms offer pharmaceutical companies the opportunity to use the findings and results that academic experiments have yielded. Sometimes firms exploit those data to further the research that they’re are already doing; other times they want to get a leg up on a research program into a new field in which they lack expertise. Companies may also want to buy up specific compounds and therapies that have shown promise in early experiments.
In addition, technological advances in recent years have opened up new avenues of exploration that companies want access to. Whether it’s artificial intelligence, sophisticated cellular techniques, or gene therapies, drugmakers are looking for help in exploiting these developments. “Both biology and chemistry, as fields, have widened a lot in recent years,” says Michelle Arkin, a chemical biologist who works with Hart as codirector of the Small Molecule Discovery Center at UCSF. “There’s a real enthusiasm in the pharma companies to take advantage of this.”
This sentiment is echoed by Carsten Schultz, a social scientist at Christian Albrechts University of Kiel whose research has investigated the effects of university-industry collaborations on research and development performance. “Even the big pharmaceutical companies need to leave old fields of activity and engage in new fields like biotechnology and cell therapies,” he says. “Pharma needs to invest in these new technologies in the medium term, but they really need academics to get ahead on the knowledge.”
Who benefits?
An optimist would say these partnerships are a way for both sectors to bring their strengths to bear: academics get more funding, pharmaceutical companies get reduced risk and more expertise, and patients get more drugs. The skeptic would say that big pharma is offloading the risk burden onto academic researchers—and the public agencies that fund them—while enjoying the fruits of their labor when things do work out.
“If you consider this from the societal part of things, the question is who takes the financial burden,” Schultz says. “Whether a university or researcher makes money depends on the system. In Germany we still have a very traditional academic system. Legally, whatever happens at the university belongs to the university.” That makes spinout companies a challenge to establish, although Schulz says there are efforts to improve this.
Even if a university administration is open to the idea of its scientists starting a business, each agreement for an academic working with a pharmaceutical company is unique. “The devil is in the details,” Arkin says. “It can be exploitative, but it can be mutually beneficial.” It’s important that scientists on both sides openly discuss what they want to get from the collaboration before any draft agreement is drawn up, she adds. “As soon as the contract writers become involved, it will be more adversarial, but if scientists on either side generally have a shared vision, that’s a good start.”
Not all agreements are created equal, and academic researchers can have various degrees of engagement. “We’ve done many collaborations where we’re so involved that we go to all [the company] team meetings, and we discuss everything with them,” Arkin says. “And then sometimes we just get paid for what we do as contractors and never really find out exactly what they do with our results. Sometimes they keep the drug target a secret from us. It just makes supplementary income for our research.”
There’s no right or wrong way to do it, but researchers should just think about what they want before signing, according to Arkin. “There’s cheap money and expensive money,” she says. “Don’t get involved in the expensive money that sees you doing things you don’t want to do or aren’t interested in.”
Why drug development has become so expensive
Drugs are getting more expensive for patients, insurers, and governments. Critics say that is down to a desire for bigger profits, but costs for pharma companies are also increasing.
A 2020 study comparing the revenues of 35 large pharmaceutical companies with those of 357 other large firms in the S&P Index showed that the former had an average profitability rate of 13.8% compared with just 7.7% for the latter.
But it’s also true that progressing a new drug from the initial stages of molecule discovery through packaging and product placement has never been more expensive. Studies estimate that the average research and development costs for a new drug range from $314 million to $2.8 billion, depending on factors that include target disease and failure rate, and whether the drug has an entirely new unique mode of action or not. Drug companies argue that these rising costs are cutting into their margins.
You can see evidence of that in the number of research site closures, says Magid Abou-Gharbia, founding director of Temple University’s Moulder Center for Drug Discovery Research. Staff layoffs accompany this trend. Bristol Myers Squibb expects to cut 2,200 jobs by year-end. Novartis laid off 29 employees in San Diego and expects to drop a further 100 jobs as it winds down its research site there. Takeda cut 440 workers from its staff in July, and the list goes on.
Recent years have also seen a flurry of corporate restructuring, which can mask the industry consolidation, Abou-Gharbia says. “When I started out there were 50-plus big pharma companies, but through mergers and acquisitions, it’s gone down to about 10. They call it synergy, but it’s really downsizing.”
There are many other interlinked factors behind increasing costs. Inflationary pressures are certainly one, as is cutting-edge science. Gene and cell therapies, for example, require expensive technology and equipment that pharmaceutical companies don’t necessarily have—so as science advances, so do the overhead costs.
Growing red tape is another contributor. “Regulatory agencies like the US Food and Drug Administration and [the European Medicines Agency] are asking for more and more paperwork and hurdles to get approval,” says Fernando Albericio, a research professor and organic chemist at the University of KwaZulu-Natal.
This bureaucratic burden means clinical trials take longer and cost more. In 2018, the Tufts Center for the Study of Drug Development investigated the amount of time drugs spend in clinical trials before an approval is granted. Between 2008 and 2013, the average was 83 months; that figure rose to 90 months between 2014 and 2018.
The good news for pharmaceutical companies is that data from a 2024 Deloitte analysis give reasons to believe the industry is turning a corner. The report measures the return on investment from the research efforts of 20 large biopharma companies. The return on investment last year was 4.1%, a significant bump from the all-time low of 1.2% the year before. The hope is that investments in new technologies such as artificial intelligence will start to yield results and sustain this recovery.
Credit: cen.acs.org
World First: Stem Cells Reverse Type 1 Diabetes in Clinical Trial
Team Metabolic Health
Most people with type 1 diabetes cannot reverse their autoimmune disease or put it into spontaneous remission – all they can do is manage their blood sugar levels with insulin, a healthy diet, and regular exercise.
Now, the successful treatment of the condition in a young woman in China has brought the possibility of a universal cure tantalizingly close.
In June 2023, doctors injected the equivalent of roughly 1.5 million insulin-producing cells into the patient’s abdominal muscles. The community of cells was carefully reprogrammed from her own stem cells.
Two and a half months later, the woman’s lifelong dependence on injected insulin came to an end – completely reversing her long-term, hard-to-control diabetes.
More than four months after the transplantation, her body was producing enough insulin on its own to keep her in a safe blood glucose range for more than 98 percent of the day.
If this one patient can keep producing insulin naturally in the coming years, she could one day be declared ‘cured’ – the first successful case of its kind in the scientific literature.
“That’s remarkable,” diabetes researcher Daisuke Yabe, who was not involved in the research, told Nature reporter Smriti Mallapaty.
“If this is applicable to other patients, it’s going to be wonderful.”
Researchers in China are already planning to open up their trial to new patients.
Type 1 diabetes occurs when the body’s immune system attacks clusters of cells in the pancreas that produce insulin, called islets.
Transplanting islets or an entire pancreas from a donor to a patient with type 1 diabetes can prove curative in some selective cases, but it is an extreme and potentially dangerous option, and there are too few donors to make it accessible for the millions of those with this autoimmune disease worldwide.
For over two decades now, scientists have tried to coax cells from fully-developed adult tissue types back into a blank state known as an induced pluripotent stem cell, and in turn, transform them into insulin-producing cells.
Figuring out how to do that with accuracy, however, is tricky work. The final product doesn’t always match real pancreatic islets.
Researchers in China have taken a new route that they say allows them greater control. Instead of introducing proteins to the stem cells, which trigger certain gene expressions, reprogramming the adult tissues into the blank state, the team has engineered induced pluripotent stem cells using small molecules.
After testing the technique in mice and non-human primates with success and safety, the team of researchers got their approval for a human clinical trial. The trial is ongoing, and three people are currently enrolled.
One of those patients is a 26-year-old woman, who was diagnosed with type 1 diabetes at age 14, and her results from one year in the trial have now been published.
Previously, this patient had already had a pancreas transplant for severe hypoglycemia, but the organ had to be removed due to “severe thrombotic complications”.
So far, her stem cell transplant seems to be working better, alongside her immunosuppressive drugs.
The findings join several other recent clinical trials that suggest further studies on stem cell transplantations are warranted.
In a trial in the US, for instance, a dozen patients with type 1 diabetes were injected with islets, created from donated stem cells. The group was also treated with immunosuppressants. All 12 participants began producing insulin naturally when glucose entered their bloodstream, according to preliminary results.
“Overall,” write the researchers in China, “the findings support further clinical studies in this direction and mark a step forward in achieving the potential of personalized cell therapy… to treat disease.”
The study was published in Cell.
Credit: sciencealert.com
Gene-editing drugs are moving from lab to clinic at lightning speed
Team Metabolic Health
One autumn day in 2020 Patrick Doherty was walking his dog up a steep mountain in County Donegal, Ireland, when he noticed he was, unusually for him, running out of breath. The eventual diagnosis was terrifying: amyloidosis, a rare genetic disease that caused a protein, amyloid, to build up in his organs and tissues. The prognosis was even worse: it would cause him years of pain until it finally killed him. In the face of such terrible fortune, though, Mr Doherty had a stroke of luck. He was able to join a trial of a new medical therapy and, with just a single injection, was apparently cured. Now, he continues to walk his dog up that steep mountain in County Donegal every week.
Scientists have already used gene editing to improve the vision of people with an inherited condition that causes blindness. Image: Pixabay
The treatment edited Mr Doherty’s genes using CRISPR-Cas9, a technology that has moved from lab to clinic at lightning speed. Scientists have already used gene editing to improve the vision of people with an inherited condition that causes blindness. They also appear able to cure sickle-cell disease with it, and to restore hearing in deaf mice. This new class of medicines will gather pace in the coming year, tackling cardiovascular disease and cancer. A new generation of more precise and efficient gene-editing tools is also undergoing trials.
CRISPR-Cas9 acts like a pair of molecular scissors that cuts DNA at a precise location. A piece of RNA (a single-stranded version of DNA) attached to the medicine guides the cutting enzyme, Cas9. Once DNA is cut, the cell’s natural repair mechanisms swing into action. Gene-editing medicines commandeer those natural cellular systems and end up replacing an existing (problematic) segment of code with a new (corrected) sequence.
The speed of innovation has been impressive. CRISPR-Cas9 was discovered in the lab in 2012 and just three years later eGenesis, a biotech firm in Cambridge, Massachusetts, had used it to edit pig embryos to create organs more suitable for transplantation into humans. By 2016 a CRISPR-Cas9 therapy was approved for testing in patients with cancer, albeit on immune cells that had been removed from the body, edited to help these cells fight the cancer better, and then returned.
The following year, Vertex and Crispr Therapeutics, pharmaceutical companies based in Boston, Massachusetts, and Zug, Switzerland, said they would co-develop a treatment named CTX001, a treatment for two disorders: sickle-cell disease and beta thalassemia. Both are caused by genetic faults in the instructions for making haemoglobin, a protein that helps red blood cells carry oxygen.
CTX001, known today as Casgevy (exagamglogene autotemcel), arrived on the market in November 2023, priced at $2.2m for a one-time treatment. It involves collecting blood stem cells from a patient, editing a gene within them to restart the production of a type of haemoglobin that is usually produced only when a baby is in the womb, and re-injecting those stem cells. The patient is then capable of creating enough healthy red blood cells to treat the symptoms of their blood disorders.
As good as it is, CRISPR-Cas9 has limitations. The RNA guide molecule can sometimes be imprecise, leading to unintended cuts to a patient’s DNA. Moreover, because the tool breaks both strands in a DNA helix, the subsequent repair can also introduce unwanted insertions or deletions. Damage to genetic information like this could eventually lead to cancer or disrupt cellular function in other ways.
Updates to the technology are thus in the works. CRISPR-Cas9 nickases, for example, are enzymes that cut only one strand of the DNA double helix. To make genetic changes, nickases therefore need to be used in pairs, meaning less risk of off-target effects. It is unlikely that both nickases in an edit would bind incorrectly to the same section of DNA. Another method, “base editing”, can chemically change a single letter of a DNA’s sequence into another without the need for cuts.
Some of these techniques are already in the clinic. In 2022 a patient with familial hypercholesterolaemia was given an infusion of a base-editing treatment as part of a trial. The disorder, which affects one in 250 people, results in reduced clearance of bad cholesterol from the blood. The treatment, VERVE-101, made by Verve Therapeutics, turns off the PCSK9 gene in the liver by making a single-letter change in the DNA (from A to G).
Beam Therapeutics, based in Cambridge, Massachusetts, is using base editing to make therapies for a range of conditions. These include making four DNA-letter changes to immune cells so that they are better able to attack leukaemia, as well as a product that works for the same diseases as Casgevy. The company reckons its base-editing drug will work better than CRISPR-Cas9 and deliver higher levels of haemoglobin. Data from early trials of base-editing technology in patients are expected in the second half of this year.
At the clinical frontier is “prime editing”, which uses a Cas9 nickase along with a specially designed RNA guide that not only locates the correct region of DNA, but also carries a template of the desired change. Also attached to the CRISPR protein is an enzyme called reverse transcriptase. This reads the RNA template and synthesises the correct DNA sequence at the location of the nicked site, giving a precisely edited gene.
In April David Liu, a molecular biologist at Harvard University, posted on X that the first trial to use prime editing in a patient had been approved only four and a half years after his lab had published the first paper on the technology. Prime Medicine, a biotech firm in Cambridge, Massachusetts, has already begun clinical trials of its drug PM359 for the treatment of chronic granulomatous disease—a life-threatening condition that affects the blood’s ability to destroy infections.
Being able to change larger pieces of the genome, as is the case with prime editing, makes it possible to treat diseases where errors stretch over a long distance, like Huntington’s disease. But it could also help with the tricky economics of treating rare diseases. Instead of making a medicine that treats a single mutation to a gene, it would be possible to fix many types of mutation with one correction. The flexibility of the technology means that, in theory, prime editing could correct almost 90% of disease-causing genetic variations.
The technological progress in gene-editing tools has not stopped. Yet another method, known as “bridge RNA”, details of which were published in Nature in June, uses a form of guide RNA that recognises two stretches of DNA—the target site and the new gene that is to be inserted. This new technique allows large stretches of DNA to be added, removed or inverted.
All these new technologies face technical and safety hurdles in the years ahead. A big question is how to deliver therapies to the right place in the body. Blood cells, cancers, the retina and the liver are all easy to reach and edit. The brain and lungs are more difficult. One solution to the delivery problem, proposed by Aera Therapeutics of Cambridge, Massachusetts, is a capsid, a nanoparticle with a protein shell. Based on human proteins, these nanoparticles could be targeted to different tissues while also not provoking a strong response from the body’s immune system.
But perhaps the biggest challenge will be economic. So far, the new generation of genomic medicines have been eye-wateringly expensive—a shot of Hemgenix, a haemophilia B gene-therapy, costs $3.5m, around a million dollars more than Casgevy. Firms believe they can charge high prices not only because of the costs of developing and making the drugs, but because they offer potentially lifelong benefits (although the durability of these treatments remains to be proved).
There are reasons to think costs might come down in time. Treating diseases that affect larger patient groups, such as heart disease, would help reduce costs. Ultimately, many believe gene-editing tools will evolve into “platforms”, where the core technology would remain unchanged and only the specific instructions for changing genes would be tweaked for new diseases. This would reduce the need for clinical trials for every new drug. Until that happens, though, firms may be forced to drop even promising treatments because of market conditions. Yet gene editing is moving so fast that it seems only a question of when, not if, these new medicines will overcome their difficulties.
© 2024, The Economist Newspaper Limited. All rights reserved. From The Economist, published under licence. The original content can be found on www.economist.com
Credit: Live Mint
Weight loss and diabetes – Know each and everything
Team Metabolic Health
Weight is a sensitive issue for many people and getting to an ideal, healthy weight is easier said than done. But when you have diabetes, there are huge benefits to losing weight if you’re carrying extra weight.
You’ll have more energy and you’ll reduce your risk of serious complications like heart disease and stroke. Losing weight can help with your diabetes control too. And if you have type 2 diabetes, losing weight could even mean going into diabetes remission.
But millions of people with diabetes find keeping to a healthy weight a huge struggle. You’re not alone in this, there’s support out there to help – a good first step is to ask your healthcare team for help and advice.
Around 60% of people with type 1 diabetes and around 85% of people with type 2 diabetes are carrying extra weight or are living with obesity.
Benefits of losing extra weight
There are so many benefits to losing extra weight – both physically and emotionally.
Extra weight around your waist means fat can build up around your organs, like your liver and pancreas. This can cause something called insulin resistance. So losing this weight could help the insulin you produce or the insulin you inject work properly.
And as you start to lose weight and get more active, you and your healthcare team may need to look at your medication, especially if you treat your diabetes with insulin or sulphonylurea. This might mean reducing the dose or making other adjustments, but talk to your healthcare team about it. For some people, needing fewer diabetes medications is a great motivation for losing weight.
Although getting type 1 diabetes has nothing to do with weight, losing any extra weight will help you reduce your risk of complications and could mean injecting less insulin.
And if you have type 2 diabetes, losing around 5% of your body weight can have real benefits for your health. If you have obesity, you are more likely to put your diabetes into remission if you lose a larger amount of weight, 15kg (or 2 stone 5lbs), as quickly and safely as possible following your diagnosis. This could mean coming off your diabetes medication completely – a life-changing possibility. This is even more likely if you lose the weight nearer to your diagnosis and quickly. It’s a myth that losing weight slowly is better for you.
Most people say they also feel better in their mood, have more energy and sleep better.
We’ve got lots of information to help you maintain a healthy weight too, to help keep you on track and prevent putting weight back on.
“We know that losing even 5% of your weight helps improve blood pressure and cholesterol levels. This can have a big impact on your overall health and go a long way to reducing your risk of serious complications, like heart disease and stroke.”
Douglas Twenefour, our Deputy Head of Care and dietitian
What’s a healthy weight to aim for?
Before you get started, you need to know what a healthy weight is and what numbers you’re aiming for. This is about working out your Body Mass Index (BMI) and your waist size.
Know your weight
Research shows that the more weight you lose, the greater the health benefits, but even losing just 5% of extra weight will improve your health.
BMI uses your height and weight to work out if you’re a healthy weight. It doesn’t look at how much fat you have around the middle, so that’s why you need to measure your waist too. You can work your BMI out for yourself using this NHS tool – it will show you your target range.
For many people living with obesity, aiming for a healthy BMI may not be realistic.
Know your waist size
- A healthy waist size depends on your gender and ethnicity. It should be:
- less than 80cm (31.5in) for all women
- less than 94cm (37in) for most men
- less than 90cm (35in) for South Asian men.
- Here’s our community champion Rohit to show you how to measure your waist.
Can diabetes cause weight gain?
If you have type 1 diabetes, when you start taking insulin, you might start to put on weight. There are lots of reasons for this, like how much insulin you take, your diet and the type of insulin you’re taking.
Insulin is a growth hormone, and any growth hormone you take will mean putting on more weight. When you’re diagnosed with diabetes it’s also likely that you lost a lot of weight in a short space of time, as this is one of the symptoms, and the weight gain is part of the recovery.
The type of insulin you take can affect your weight in different ways. We’ve got more information about the different types and how they can affect your weight.
If you’re worried about putting on weight, or you’d like some help losing weight, then we’re here to help.
Diabetes diet plans to lose weight
- You may have heard that diabetes can be controlled by diet. There is no such thing as a special diet exclusively for people with diabetes. There are a lot of different ways to lose weight – but there’s no one-size-fits-all diet.
- It starts with finding a way to eat fewer calories than you need.
- A calorie (or kcal) is a unit of energy, which is in the food and drink we consume. Your body uses energy for everything we do – from breathing and sleeping to exercising. When you eat, you’re replacing the energy you’ve used, which helps you to maintain a healthy weight.
- As a general guide, government recommendations are that men need around 2,500kcal a day to maintain a healthy weight, and women need around 2,000kcal a day. But most people need different amounts of calories based on how their bodies work, how active they are and any weight management goals.
We’ve put together some 7-day meal plans to help you lose weight. They’re all clinically approved, nutritionally balanced, calorie and carb counted, and can help if you want to lose weight:
- Low-carb diet plan
- Mediterranean diet plan
- Lower-calorie diet plans, like 1,200 or 1,500 calories a day
- Evidence shows that the best approach is the one that you’re likely to stick to. So the key is to find a plan that you enjoy and fits in with the rest of your life. Everyone’s different and what works for some may not for others.
Low-calorie and very low-calorie diets
A low-calorie diet is made up of between 800 to 1200 calories a day – our DiRECT study used a low-calorie diet of around 850 calories a day to see if type 2 diabetes could be put in to remission. But DiRECT is not a diet. It’s a weight-management programme, delivered in GP practices in some areas of the country.
Then there’s a very low-calorie diet, which means having less than 800 calories a day.
We haven’t created low or very-low calorie meal plans as these could be challenging for most people to make themselves at home. Most people who follow these diets use special meal replacement products, likes soups and shakes, which are nutritionally complete. If you chose to try a low-calorie diet like the one in DiRECT, speak to your GP or nurse first, especially if you use medications like insulin.
Other diets
A low GI diet can help you manage your blood sugar levels, but the evidence for people with diabetes losing weight is not very strong.
There are other popular diets, like intermittent fasting (such as the 5:2 diet) and the Paleo diet. Unfortunately there isn’t enough strong evidence to say these are effective for weight loss in people with diabetes either.
Commercial weight-loss programmes
Some people feel that they need more support and choose to join a commercial weight-loss programme. These usually involve calorie-controlled eating plans or meal replacements, like milkshakes or bars.
It’s really important to ask lots of questions about these programmes, so you’ve got all the evidence and information you need to make an informed decision. Here are some ideas:
- Has a healthcare professional been involved?
- Does the programme offer advice on your diabetes (especially if you’re at risk of hypos)?
- Are you getting all the nutrition you need from this programme?
Does the programme give support and education?
Whether you choose to try one of our meal plans, or another type of diet, it’s really important that you talk it through with your diabetes team first. Starting a new diet will affect your medication or blood sugar levels, so you need their knowledge and support.
Weight-loss planner
“I keep a daily diary and log my weight and activity. It keeps me accountable and focused.”
Edward Morrison
You can download My weight-loss planner (PDF, 534KB) to set goals and track your progress. By putting a plan in place and noting down your progress, you’ll be able to see the positive changes you’re making.
Your feelings about food
The emotional part of trying to lose weight is important and can often be overlooked.
Do you feel guilty when you eat a treat? Do you eat more when you’re upset? Do you feel dejected if you can’t see progress straight away?
These are really common feelings and tackling them can help you on the road to a healthier lifestyle and a healthy weight.
Find out more about your feelings about food and diabetes.
Connect with others and share tips in our online forum – we’ve made a board especially for people who are looking to lose weight.
Exercise and being active for weight loss
Regular exercise or physical activity has many health benefits and will help you in your weight loss journey. We’ve got more information about how much activity you should be doing and different ways to get active.
But before you start any new physical activity, speak to your diabetes team. They can make sure you have all the information you need about how your diabetes might be affected. Especially if you treat your diabetes with insulin or certain diabetes medications like sulphonylureas, as being more active may increase your risk of hypos.
Your diabetes team will support you to make the right adjustments to your medications to reduce your risk of hypos.
Weight loss surgery
If you have a lot of weight to lose, ask your healthcare team if weight loss surgery is a possibility. There are different types of weight loss surgery, also called bariatric surgery. They aim to make you feel fuller sooner and eat less. Weight loss surgery can be a very effective way of losing weight, keeping your HbA1c in the target range and putting type 2 diabetes into remission for some people.
For people with diabetes, weight loss surgery isn’t just about weight loss. It is now seen as an actual treatment for type 2 diabetes, and the weight loss is a bonus.
Weight loss surgery changes the way the digestive system works, in ways that are helpful for people with type 2 diabetes. It can:
- change how the hormones in your gut work, which in turn affects how your body makes insulin
- increase the amount of bile acids that your body makes, these make your body more sensitive to insulin
- improve the way your body uses insulin, leading to lower blood sugar levels.
Diabetes weight loss medication
Your healthcare team may be able to prescribe some weight loss medications which can help with weight loss. One of these is Orlistat. Some diabetes medications, such as GLP-1 analogues, can also help with weight loss
Your healthcare team can give you advice about whether these medications are right for you. Avoid buying medications online and always get advice from a healthcare professional
Credit: diabetes.org.uk
Lilly releases Zepbound® (tirzepatide) single-dose vials, expanding supply and access for adults living with obesity
Team Metabolic Health
Eli Lilly and Company (NYSE: LLY) today announced Zepbound® (tirzepatide) 2.5 mg and 5 mg single-dose vials are available for self-pay for patients with an on-label prescription, significantly expanding the supply of Zepbound in response to high demand. The single-dose vials are priced at a 50% or greater discount compared to the list price of all other incretin (GLP-1) medicines for obesity. This new option helps millions of adults with obesity access the medicine they need, including those not eligible for the Zepbound savings card program, those without employer coverage, and those who need to self-pay outside of insurance.
“We are excited to share that the Zepbound single-dose vials are now here, further delivering on our promise to increase supply of Zepbound in the U.S.,” said Patrik Jonsson, executive vice president, and president of Lilly Cardiometabolic Health and Lilly USA. “These new vials not only help us meet the high demand for our obesity medicine, but also broaden access for patients seeking a safe and effective treatment option. In a clinical study, the 5 mg maintenance dose helped patients achieve an average of 15% weight loss after 72 weeks of treatment and has been a powerful tool for millions of people with obesity looking to lose weight and keep it off.”
Lilly has created a new self-pay pharmacy component of LillyDirect where patients with a valid, on-label prescription from the health care provider of their choice can purchase the vials. Distributing the vials via this channel ensures patients and providers can trust they are receiving genuine Lilly medicine, building on the company’s efforts to help protect the public from the dangers posed by the proliferation of counterfeit, fake, unsafe or untested knock-offs of Lilly’s medications. Lilly has also taken a vocal stance against the use of obesity medicine for cosmetic weight loss; a multi-step verification process will help ensure the vials are dispensed only to patients who have a valid, on-label electronic prescription from their health care provider. Patients can also purchase ancillary supplies, like syringes and needles, and will have access to important patient-friendly instructional materials on correctly administering the medicine via needle and syringe.
“People living with obesity have long been denied access to the essential treatment and care needed to manage this serious chronic disease,” said James Zervos, chief operating officer, Obesity Action Coalition. “Expanding coverage and affordability of treatments is vital to people living with obesity. We commend Lilly for their leadership in offering an innovative solution that brings us closer to making equitable care a reality. Now, it’s time for policymakers, employers and insurers to work with pharmaceutical companies to ensure no one is left behind in receiving the care they deserve and need.”
A four-week supply of the 2.5 mg Zepbound single-dose vial is $399 ($99.75 per vial), and a four-week supply of the 5 mg dose is $549 ($137.25 per vial) – less than half the list price of other incretin medicines for obesity and in line with the Zepbound savings program for non-covered individuals. The self-pay channel enables a transparent price by removing third-party supply chain entities and allowing patients to access savings directly outside of insurance.
“Despite obesity being recognized as a serious chronic illness with long-term consequences, it’s often misclassified as a lifestyle choice, resulting in many employers and the federal government excluding medications like Zepbound from insurance coverage,” said Jonsson. “Outdated policies and lack of coverage for obesity medications create an urgent need for more innovative solutions. Bringing Zepbound single-dose vials to patients will help more people living with obesity manage this chronic condition. We will also continue to advocate for a system that better aligns with the science.”
In a clinical study, tirzepatide 5 mg, along with a reduced calorie diet and increased physical activity, achieved an average of 15% weight loss over 72 weeks compared to 3.1% for placebo. Zepbound is the first and only obesity treatment of its kind that activates both GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1) hormone receptors. Zepbound tackles an underlying cause of excess weight. It reduces appetite and how much you eat. Zepbound is indicated for adults with obesity, or those who are overweight and also have weight-related medical problems, to lose weight and keep it off. Zepbound should be used with a reduced-calorie diet and increased physical activity. It should not be used in children under 18 years of age or with other tirzepatide-containing products or any GLP-1 receptor agonist medicines. Zepbound has not been studied in patients with a history of pancreatitis, or with severe gastrointestinal disease, including severe gastroparesis, and it is unknown if patients with a history of pancreatitis are at higher risk for developing pancreatitis on Zepbound.
Zepbound is also available in 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg per 0.5 ml doses in a single-dose pen (autoinjector). The recommended maintenance dosages are 5 mg, 10 mg, or 15 mg injected subcutaneously once weekly.
Credit: lilli.com
How carnitine transporters boost reproductive health
Team Metabolic Health
Understanding how carnitine transporters regulate sperm motility and hormone production could unlock new fertility treatments, offering hope for millions affected by infertility globally.
Carnitine transport mediated by multiple SLCs is depicted with different colors. The transport of carnitine across epithelial cells of the intestine, kidney, and placenta, as well as into the liver, brain, heart, muscle, epididymis, and airway tissues, is shown. OCTN2 (Green): mediates carnitine transport by a sodium-dependent mechanism, which is not reported for the sake of clarity. CT2 (Purple): involved in carnitine transport, specifically in the epididymis, contributing to sperm maturation. OCTN1 (Yellow): Low-affinity carnitine transporter participates in carnitine transport in various tissues. ATB0,+ (Blue): mediates sodium and chloride-dependent transport of carnitine, not reported for the sake of clarity, in the intestine and other tissues. MCT9 (Pink): transporter associated with carnitine efflux through the basolateral membrane of absorption epithelia like intestine and kidney. Arrows indicate the direction of carnitine transport across cellular membranes. Image created using Adobe Illustrator. Human transporters are represented as space-fill models from AlphaFold.
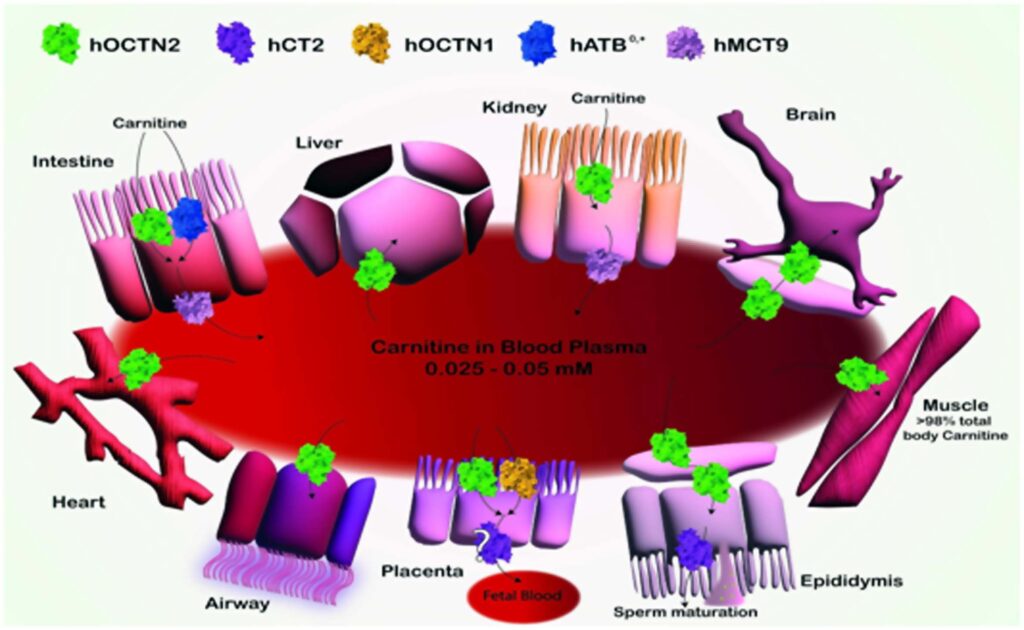
Schematic Representation of Carnitine Transport and Distribution in Various Tissues.
A recent study published in the journal Biochemical Pharmacology reviewed the role of membrane transporters in carnitine homeostasis, focusing on the molecular mechanisms involved and the implications in fertility. Carnitine is a crucial molecule in metabolism. It primarily drives fatty acid β-oxidation within mitochondria and plays a significant role in maintaining metabolic flexibility. Diet is the primary source of carnitine in humans, with only a small fraction being endogenously synthesized. The biosynthesis of carnitine requires the flux of its intermediates through different organelle membranes, and the majority of carnitine synthesis occurs in the liver, with additional synthesis in the kidneys and brain. As such, carnitine and its metabolites are distributed to tissues and organelles by membrane transporters.
Carnitine’s role in brain health: Besides fertility, carnitine is implicated in brain plasticity and cognitive functions, with acetylcarnitine influencing gene expression through histone acetylation.
The primary carnitine shuttle system in mitochondria comprises two enzymes (carnitine palmitoyl transferase 1 [CPT1] and CPT2) and an inner mitochondrial membrane transporter, carnitine/acylcarnitine carrier (CAC), also known as solute carrier 25 member 20 (SLC25A20). CAC is crucial for transporting acylcarnitines into mitochondria for β-oxidation. Notably, no redundant mitochondrial transporter compensates for CAC deficiency, making it indispensable for cellular life. Other carnitine shuttles are active in the endoplasmic reticulum and peroxisomes.
The coordination of peroxisomal and mitochondrial carnitine shuttles is essential for fatty acid catabolism. Carnitine has been implicated in modulating the acetyl-coenzyme A (CoA)-to-CoA ratio, which profoundly impacts lipid biosynthesis, gene expression, and carbohydrate metabolism. In the present study, researchers reviewed the role of transporters in carnitine traffic, focusing on the relationship between carnitine and fertility.
Carnitine network and alterations
Carnitine distribution is highly variable across tissues, ranging from low millimolar levels in most tissues to the highest (60 mM) in the testes. Many transporters are involved in maintaining carnitine homeostasis. Diet plays a crucial role in carnitine distribution; in fish and meat consumers, dietary carnitine accounts for about 75% of the total carnitine content. In contrast, vegans and vegetarians often rely heavily on endogenous synthesis and renal reabsorption for maintaining carnitine levels. Without supplements, vegans and vegetarians may experience reduced carnitine levels.
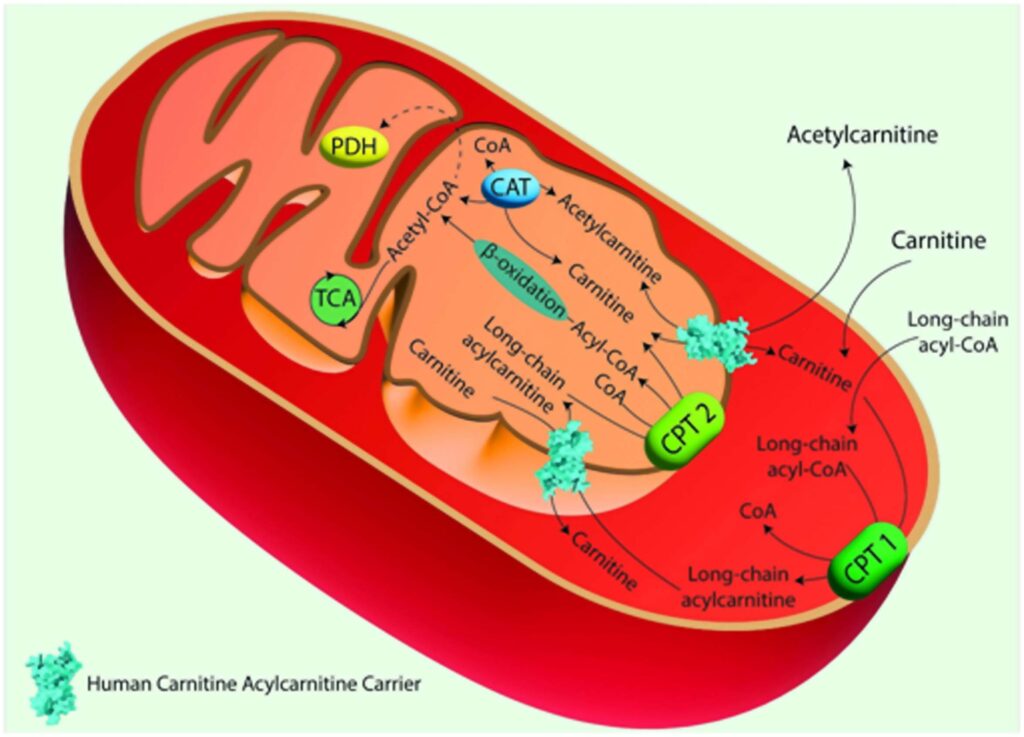
The Carnitine Shuttle in Mitochondrial Fatty Acid Oxidation.
Acyl-CoA synthase catalyzes the conversion of long-chain fatty acids into fatty acyl-CoAs. These are then converted to acylcarnitines by Carnitine Palmitoyl Transferase 1 (CPT 1), which is located in the outer mitochondrial membrane. Acylcarnitines are transported across the inner mitochondrial membrane by the Carnitine/Acylcarnitine Carrier (CAC) in exchange for free carnitine. Once inside the mitochondrial matrix, Carnitine Palmitoyl Transferase 2 (CPT 2), located on the inner mitochondrial membrane, converts acylcarnitines back into acyl-CoAs and free carnitine. The free carnitine is transported to the cytosol by the CAC, and it can be recycled by CPT 1. The acyl-CoAs imported into the mitochondrial matrix through the carnitine shuttle are subjected to β-oxidation, producing acetyl-CoA, which can then enter the TCA. Image created using Adobe Illustrator. hCAC is represented as space fill model from AlphaFold prediction
As such, endogenous synthesis and reabsorption may be more relevant for homeostasis. Renal reabsorption of carnitine is the primary means of compensating for dietary carnitine deficiencies. Organic cation/carnitine transporter 2 (OCTN2) facilitates carnitine reabsorption in the kidneys; mutations in OCTN2 lead to primary carnitine deficiency (PCD), a disorder characterized by systemic carnitine depletion and associated clinical manifestations, including muscle weakness, cardiomyopathy, and infertility. PCD treatment involves lifelong carnitine supplementation.
Carnitine deficiency in autism: Mutations in enzymes involved in carnitine biosynthesis have been linked to autism spectrum disorders, indicating a broader systemic impact of carnitine beyond fertility.
Secondary carnitine deficiencies (SCDs) may occur due to inherited defects in CPT2, CAC, or acyl-CoA dehydrogenases. Notably, CAC defects often result in life-threatening conditions due to impaired mitochondrial β-oxidation, leading to increased fatty acid accumulation in the cytoplasm. There are no redundant carnitine transporters to compensate for CAC defects. Therefore, early intervention is paramount for CAC deficiency. Treatment strategies for SCDs include diet-induced hypoglycemia prevention, carnitine supplementation, and medium-chain fatty acid diets.
Carnitine and Oxidative Stress in Infertility
Oxidative stress plays a pivotal role in both male and female infertility, with reactive oxygen species (ROS) and reactive nitrogen species (RNS) contributing to lipid peroxidation, DNA fragmentation, and reduced sperm viability. Carnitine, with its antioxidant properties, helps mitigate oxidative damage by scavenging free radicals, protecting sperm mitochondria from oxidative stress, which is particularly important in the preservation of sperm motility and overall fertility. The study also highlights how the antioxidant function of carnitine is crucial in managing oxidative stress in female reproductive tissues, such as the ovaries, where ROS imbalances can impair oocyte quality and disrupt the endometrial environment.
Human infertility
Globally, infertility is a significant concern, affecting over 180 million couples. Historically, it was predominately attributed to females; however, contemporary insights highlight a significant male contribution. The cause of infertility remains unexplained in many cases despite diagnostic advances. Mitochondrial dysfunctions are emerging as a common factor in both male and female infertility, linking energy metabolism to reproductive health. Lifestyle choices influence fertility, with evidence linking alcohol, obesity, and smoking to poor semen quality and ovulatory function.
Further, despite multiple studies on the relationship between male fertility and carnitine, the underlying molecular mechanisms remain elusive. In the male reproductive system, carnitine facilitates mitochondrial energy metabolism, particularly by regulating the acetylcarnitine/CoA ratio, which putatively is responsible for sperm concentration and motility. This regulation is particularly important in sperm maturation, where carnitine concentrations increase dramatically from the epididymal head (5 mM) to the tail (60 mM).
Some studies have suggested that lumen carnitine may stabilize the plasma membrane of sperms, enhance survival, and mitigate acrosome-reacted sperms, which are critical for successful fertilization.
The role of carnitine in females is less clear. However, carnitine is involved in the energy supply necessary for ovulation, folliculogenesis, and embryonic development. Mitochondrial dysfunction, exacerbated by carnitine deficiency, has been implicated in conditions like polycystic ovary syndrome (PCOS) and endometriosis. Therefore, carnitine deficiency could result in suboptimal energy, compromising oocyte quality and reducing the fertilization potential. Furthermore, carnitine has been shown to influence the production of sex hormones such as testosterone, estrogen, and progesterone, which are crucial for reproductive health.
SLCs in the carnitine network
Studies indicate that OCTN1 might function as a carnitine transporter in tissues with high carnitine levels, such as the epididymis. However, direct links between OCTN1 and infertility have not been studied so far. OCTN2 is the highest-affinity carnitine transporter. It is ubiquitously expressed in the heart, skeletal muscle, kidneys, and intestine. Mutations in OCTN2 are associated with Crohn’s disease (CD) due to carnitine deficiency in the intestinal epithelium. Further, mutations in OCTN2 can lead to fertility issues by disrupting carnitine homeostasis in the reproductive system, particularly in the epididymis. In the male reproductive system, carnitine transporter 2 (CT2) is localized in the luminal membrane of epididymal cells and the plasma membrane of Sertoli cells in the testes. In females, CT2 is highly expressed in the endometrium.
CT2 localization in the testes is the primary molecular link between male infertility and carnitine; however, its presence in the endometrium or testes does not clarify whether carnitine is associated with transporter regulation or energy requirements. CAC is an indispensable protein for cellular life. While the study points to CAC’s potential role in infertility, no direct causal mutations linking CAC to fertility dysfunction have been confirmed yet.
Clinical Implications
The study concludes by suggesting potential treatment avenues. Carnitine supplementation has shown promise in improving sperm motility and morphology in idiopathic infertility cases, while its role in antioxidant defense highlights its therapeutic potential in oxidative-stress-related reproductive disorders. Recognizing the role of carnitine and SLCs in sperm motility and energy metabolism could help develop advanced, more refined diagnostic tools and targeted therapies. Further research is necessary to understand the exact molecular mechanisms linking carnitine transporters and reproductive health, which could lead to novel treatments for both male and female infertility.
Credit: news-medical.net
GLP-1 drugs protect brain health by improving neurovascular function and reducing inflammation
Team Metabolic Health
New research reveals how GLP-1 receptor drugs, known for treating diabetes and obesity, also protect the brain’s vital neurovascular system, offering hope for tackling cognitive decline and neurodegenerative diseases like Alzheimer’s.
In a recent review published in the journal Cell Metabolism, a group of authors explored how Glucagon-Like Peptide-1 receptor (GLP-1R) agonism shapes the neurovascular unit (NVU), potentially linking metabolic health improvements to enhanced brain health.
Background
GLP-1R agonists protect the blood-brain barrier (BBB): These drugs help maintain the integrity of the BBB by preventing tight junction degradation, which can reduce the risk of neuroinflammation and cognitive decline.
Overconsumption of readily available, nutrient-rich foods has created an environment of overnutrition, leading to health issues like obesity and metabolic syndrome. Chronic low-grade inflammation, often associated with obesity, contributes to neurodegenerative diseases. GLP-1R agonists have emerged as effective tools for managing weight by influencing appetite and addressing metabolic dysfunctions. GLP-1R agonism not only helps with weight management but also appears to provide neuroprotective effects, including reducing neuroinflammation and enhancing brain health. Further research is needed to clarify whether GLP-1R agonism impacts brain health directly or through improved metabolic function.
The role of GLP-1 in metabolic regulation
GLP-1 is a hormone produced both in the gut and the brain. It plays a key role in maintaining glucose homeostasis by increasing insulin secretion and reducing glucagon levels post-meal. This incretin hormone also delays gastric emptying, thereby slowing glucose absorption and preventing sharp rises in insulin levels. Beyond its metabolic functions, GLP-1 is involved in regulating various behaviors, including feeding, fluid intake, and even motivated behaviors like drug consumption. Importantly, GLP-1 receptors are found not only in neurons but also in glial cells, which mediate its effects on brain health by regulating energy balance and maintaining neural circuits.
GLP-1R agonists in obesity management
GLP-1R agonists, such as semaglutide, liraglutide, and tirzepatide, have gained prominence in the treatment of obesity. These drugs work by mimicking the action of endogenous GLP-1 but at supraphysiological doses, resulting in stronger and longer-lasting effects on appetite suppression. While endogenous GLP-1 has a short half-life and limited ability to act on distant organs, exogenous GLP-1R agonists have proven highly effective in reducing food intake and promoting weight loss.
Obesity is a significant risk factor for a range of chronic conditions, including type 2 diabetes and cardiovascular diseases. Individuals with obesity often experience chronic low-grade inflammation, which not only affects peripheral tissues but also has detrimental effects on brain health, linking obesity to neurodegenerative diseases.
Chronic inflammation, obesity, and brain health
Chronic inflammation, a hallmark of obesity, is associated with an increased risk of developing neurological conditions, including cognitive decline and neurodegeneration. The inflammatory state extends to the brain, contributing to conditions such as Alzheimer’s disease (a neurodegenerative disorder characterized by progressive memory loss and cognitive decline). This inflammatory process involves activation of microglia and astrocytes—glial cells critical for immune responses in the brain. The neuroinflammatory processes observed in obesity are similar to those seen in neurodegenerative diseases, with microglial activation, reactive astrogliosis, and insulin resistance playing key roles.
Neuroprotective effects of GLP-1R agonism
GLP-1R agonists improve cerebral blood flow (CBF): By enhancing neurovascular coupling, these drugs ensure that blood flow is properly regulated in response to brain activity, improving overall brain function, particularly in obesity and metabolic disorders.
Beyond their role in weight management, GLP-1R agonists have shown neuroprotective and neurotrophic properties, offering potential benefits in reducing neuroinflammation. GLP-1R signaling in microglia helps reverse the polarization of these immune cells from a pro-inflammatory state to an anti-inflammatory state, thus reducing neuroinflammation. GLP-1R agonism has been observed to reduce microglial activation, a key driver of neuroinflammation, and to protect against neuronal damage. Furthermore, these agonists may improve brain insulin sensitivity, reduce oxidative stress, and promote the survival of neurons.
Recent studies suggest that GLP-1R agonists may influence the neurovascular unit (NVU), the critical interface where neurons, glial cells, and blood vessels interact to maintain brain function. The NVU plays a pivotal role in ensuring proper blood flow to the brain, regulating nutrient supply, and removing waste products. Dysfunction in the NVU is linked to both metabolic disorders and cognitive decline.
GLP-1 and the NVU
GLP-1 receptors are expressed on various cell types within the NVU, including neurons, astrocytes, microglia, and endothelial cells. Activation of these receptors by GLP-1R agonists has been shown to confer protection against microvascular damage, particularly in models of diabetic retinopathy and stroke. Given the similarities between the brain’s and retina’s vascular systems, these findings suggest that GLP-1R agonism could also protect the brain’s microvasculature, preserving the integrity of the blood-brain barrier and improving cerebral blood flow.
In models of high-fat diet-induced obesity, GLP-1R agonism has demonstrated the ability to enhance neurovascular coupling, improving the relationship between neuronal activity and blood flow in the brain. This may counteract the neurovascular dysfunction caused by chronic overnutrition. These findings suggest that GLP-1R agonists may help counteract the adverse effects of overnutrition on brain health.
Implications for neurodegenerative diseases
The potential for GLP-1R agonism to protect the brain and improve cognitive function has spurred interest in its use as a therapeutic strategy for neurodegenerative diseases like Alzheimer’s. Preclinical studies have demonstrated that GLP-1R agonists can reduce the accumulation of amyloid plaques, a hallmark of Alzheimer’s disease, and improve synaptic function. In addition, GLP-1R agonists have been observed to enhance the health of endothelial cells in the brain, promoting vascular remodeling, which may further support cognitive function.
Additionally, the ability of GLP-1R agonists to modulate the NVU and reduce neuroinflammation suggests that they could slow the progression of neurodegenerative diseases. By improving the health of the brain’s vasculature and reducing inflammatory responses, GLP-1R agonists may help preserve cognitive function in individuals with metabolic disorders or neurodegenerative conditions.
Conclusions
To summarize, the connection between metabolic and cognitive health highlights brain-body communication, redefining some disorders as neurometabolic. Repurposing antidiabetic drugs like GLP-1 mimetics for neurological diseases is gaining interest, as metabolic disorders pose a significant risk for neurodegeneration. GLP-1 mimetics show promise due to their anti-inflammatory, neuroprotective, and neurotrophic properties. The expression of GLP-1R on various cell types and its impact on the neurovascular unit (NVU), including neurons, glial cells, and endothelial cells, make GLP-1 a strong candidate for bridging brain-body crosstalk.
Credit: news-medical.net
Living with obesity – and what it means for your heart and general health
Team Metabolic Health
Obesity is a risk factor for a number of complications. Some of these are cardiovascular, a group that includes coronary artery disease, high blood pressure, stroke, hyperlipidaemia, heart attack and heart failure.1 Obesity is also a leading cause of cardiovascular mortality and morbidity.1 Here is the good news: With appropriate action, supported by professional guidance and advice, the cardiovascular risk factors may be managed and reduce chance of complications.
Clarifying a few important terms
This blog post is about how obesity affects health, with a particular emphasis on so-called cardiovascular complications of obesity. The last part of that might sound a bit cryptic, so let’s begin by clarifying a few important terms. It’s actually quite simple.
“Cardio” means related to the heart, while “vascular” means related to the blood vessels.
Thus, cardiovascular complications, for instance, is simply a way to refer to a cluster of issues that primarily affect the heart and blood vessels.
Living with obesity tends to increase the risk of developing cardiovascular complications or even suffering a cardiovascular event such as stroke or heart attack.1
But consider this: Obesity doesn’t define anyone. It’s a condition and a disease for which there are genetic as well as biological, behavioural, psychosocial and environmental reasons2 – true! But that doesn’t make obesity irreversible or inescapable.
A closer look at cardiovascular complications
Obesity is a disease that increases the risk of unintended cardiovascular health consequences3. It happens to be a rather critical one. In fact, obesity is among the leading causes of elevated cardiovascular disease, mortality and morbidity1. This video might help you to understand it better:
Obesity may do more than that
Unfortunately, that’s true. In fact, obesity may increase the risk of developing over 200 complications5, including type 2 diabetes, asthma, cancer, liver and gallbladder disease, sleep apnea, osteoarthritis and gynaecological complications1.
But let’s focus on those affecting the heart and blood vessels such as ischaemic heart disease, coronary artery disease and hypertension1 – the latter being a cardiovascular risk factor in its own right, potentially leading to stroke, heart attack and heart failure.1
Admittedly, the relationship between obesity and its potential cardiovascular consequences is a serious one. But every cloud has a silver lining.
Let’s switch gears and focus instead on the…
Reasons to be hopeful
While the consequences of living with obesity could be serious, steps towards reducing your risk can be taken. Doctors trained in obesity care know what kind of action yields positive results. We are collectively much smarter about obesity today than we once were.
Many people living with obesity can, for instance, learn from a properly trained obesity care provider. But the opposite is also true. Many doctors can learn from those affected by obesity – about how different treatment strategies are experienced at the individual level, for instance, mentally and physically. You can read more about it here.
A significant step in the direction of a healthier future
The fact that the medical and scientific community have conclusively shown that obesity is a disease is really cause for celebration! Why? Because it means we are significantly closer to being able to address it optimally.
For anyone affected by obesity, reaching out to carefully trained obesity care providers for advice and guidance can make a difference. Such specialists can help outline a personalised weight management strategy – one that takes stock of obesity’s multifactorial nature and doesn’t ask more of you than is appropriate and reasonable.
Why weight loss is helpful
Doctors have found that weight loss can benefit the heart. For example, losing 5% of one’s body weight has been associated with significant and long-standing health benefits7-18. These include reduced blood pressure19, leading to improved heart health.
And while some complications are more sensitive to weight loss than others, increasing weight loss beyond 5% may lead to additional improvements in obesity-related complications7-18. In a study involving people with type 2 diabetes, weight loss of 5–10%, for instance, was shown to produce improvements in cardiovascular risk factors a year after the weight loss.
Continue – or begin – your weight management journey today!
Remember, change starts with you. But it doesn’t have to end with you – not if you do the smart thing and reach out to those who have a professional, scientific understanding of genes, metabolism, human psychology and all the other complexly interwoven factors of obesity.
By doing that, healthy change can continue to benefit you – in the form of sustained weight loss and reduced cardiovascular risk factors now and in the future.
We wish you success with your next steps to better health.
Credit: truthaboutweight.global