
Rethinking Addiction as a Chronic Brain Disease
Team Metabolic Health
Some researchers argue that the roles of social environment and personal choice have to be considered in order to make progress in treating people addicted to drugs.
The message emblazoned on a walkway window at the airport in Burlington, Vt., is a startling departure from the usual tourism posters and welcome banners:
“Addiction is not a choice. It’s a disease that can happen to anyone.”
The statement is part of a public service campaign in yet another community assailed by drug use, intended to reduce stigma and encourage treatment.
For decades, medical science has classified addiction as a chronic brain disease, but the concept has always been something of a hard sell to a skeptical public. That is because, unlike diseases such as Alzheimer’s or bone cancer or Covid, personal choice does play a role, both in starting and ending drug use. The idea that those who use drugs are themselves at fault has recently been gaining fresh traction, driving efforts to toughen criminal penalties for drug possession and to cut funding for syringe-exchange programs.
But now, even some in the treatment and scientific communities have been rethinking the label of chronic brain disease.
Pix Credit: Medar De La Cruz
In July, behavior researchers published a critique of the classification, which they said could be counterproductive for patients and families.
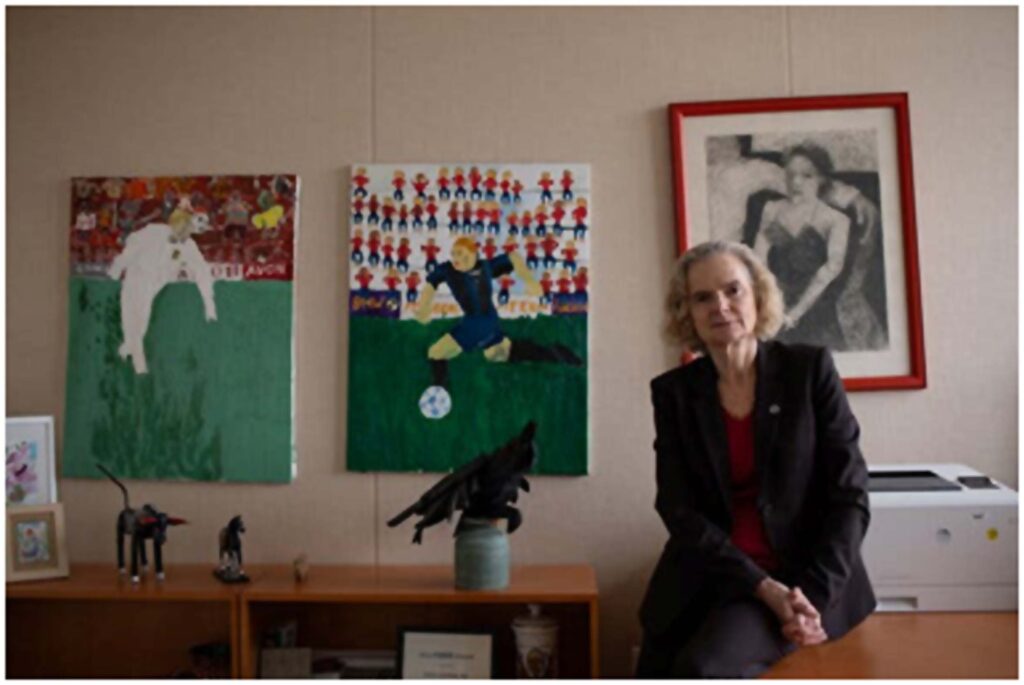
“I don’t think it helps to tell people they are chronically diseased and therefore incapable of change. Then what hope do we have?” said Kirsten E. Smith, an assistant professor of psychiatry and behavioral sciences at Johns Hopkins School of Medicine and a co-author of the paper, published in the journal Psychopharmacology. “The brain is highly dynamic, as is our environment.”
The recent scientific criticisms are driven by an ominous urgency: Despite addiction’s longstanding classification as a disease, the deadly public health disaster has only worsened.
Almost no one is calling for entirely scrapping the disease model . Few dispute that constant use of stimulants like methamphetamine and opioids like fentanyl have a detrimental effect on the brain.
But some scientists argue that brain-centric disease characterizations of addiction do not sufficiently incorporate factors like social environment and genetics. In the recent critique, researchers contended that, rather than emphasizing the brain’s brokenness in perpetuity, an addiction definition should include the motivation or context in which the person chose to use drugs.
That choice, they said, is often about seeking an escape from intractable conditions such as a fraught home, undiagnosed mental health and learning disorders, bullying or loneliness. Generations of family addiction further tip the scales toward substance use.
And in many environments, they added, drugs are simply more readily available than healthier, rewarding options, including education and jobs.

Kirsten E. Smith, an assistant professor at Johns Hopkins School of Medicine, disputes the definition of addiction as a chronic brain disease. “I am not in recovery,” she said. “I have recovered.” Pix Credit: Schaun Champion for The New York Times
Fentanyl Overdoses: What to Know
Devastating losses. Drug overdose deaths, largely caused by the synthetic opioid drug fentanyl, reached record highs in the United States in 2021. Here’s what you should know to keep your loved ones safe:
Understand fentanyl’s effects. Fentanyl is a potent and fast-acting drug, two qualities that also make it highly addictive. A small quantity goes a long way, so it’s easy to suffer an overdose. With fentanyl, there is only a short window of time to intervene and save a person’s life during an overdose.
Stick to licensed pharmacies. Prescription drugs sold online or by unlicensed dealers marketed as OxyContin, Vicodin and Xanax are often laced with fentanyl. Only take pills that were prescribed by your doctor and came from a licensed pharmacy.
Talk to your loved ones. The best way to prevent fentanyl use is to educate your loved ones, including teens, about it. Explain what fentanyl is and that it can be found in pills bought online or from friends. Aim to establish an ongoing dialogue in short spurts rather than one long, formal conversation.
Learn how to spot an overdose. When someone overdoses from fentanyl, breathing slows and their skin often turns a bluish hue. If you think someone is overdosing, call 911 right away.
Buy naloxone. If you’re concerned that a loved one could be exposed to fentanyl, you may want to buy naloxone. The medicine can rapidly reverse an opioid overdose and is often available at pharmacies without a prescription. Narcan, the nasal spray version of naloxone, has received F.D.A. approval to be sold over the counter and should be widely available by late summer.
Choosing drugs could then be understood not as a moral failing but as a form of decision making, with its own bleak logic.
Dr. Nora Volkow, director of the National Institutes on Drug Abuse, said the current model still holds value, and refers to addiction as “a chronic, treatable medical condition.” Pix Credit: Hailey Sadler for The New York Times
In combination with medications that subdue opioid cravings, therapists could help patients identify the reasons that led them to use drugs and then encourage them to make choices that result in meaningful, sustained rewards.
In a 2021 paper in the journal Neuropsychopharmacology, Dr. Markus Heilig, a former research director at the National Institute on Alcohol Abuse and Alcoholism, defended the brain-disease diagnosis, saying evidence has been amply documented. But, his paper acknowledges, “Brain-centric accounts of addiction have for a long time failed to pay enough attention to the inputs that social factors provide to neural processing behind drug seeking and taking.”
In clinical practice, the term “addiction” is becoming increasingly nuanced. John F. Kelly, a psychologist and professor of addiction psychiatry at Harvard Medical School, defines addiction as “a severe substance use disorder that is at the point where there are lots of changes in the prefrontal cortex as well as deeper areas of the brain” that regulate emotion and behavior.
But only a small minority of people meet that criteria, he said. “Even within that severe range, there’s a lot of different degrees of impairment that can occur,” Dr. Kelly added. Genetics can exacerbate the severity of the response.
He offered the analogy of boarding a speeding train. “It starts off being an exhilarating ride, but at some point it gets out of control and becomes derailed. It’s a matter of when you can pull the emergency cord and get off,” he said, noting that some drug users never get the chance to do so before it’s too late.
That moment differs for everyone: “People will only change when there are negative consequences, but also when there is hope and optimism that change is possible, likely and sustainable.”
In disputing the characterization of addiction as a disease marked by compulsive or relapsing use, a few experts have argued that some drug and alcohol users can quit without treatment — and even return to occasional safe use.
Dr. Smith began using drugs in adolescence and became addicted to heroin. During her darkest stretch, when she was 23, she was injecting four times daily. She was involved in two bank robberies and then served almost four years in federal prison, where she attended a modest treatment program. Upon release, she finished college and completed graduate and postdoctoral studies.
It has been more than six years since she used opioids and more than 15 since she was addicted to them. Dr. Smith is quick to credit the benefits of her middle-class background and family support.
She rejects the idea that she will always be shackled to a chronic brain condition.
“I am not in recovery,” she said. “I have recovered.”
Theories of addiction have been debated for centuries. In the 1780s, Dr. Benjamin Rush, a signer of the Declaration of Independence, began calling alcoholism “that odious disease.” (“The different preparations of opium are a thousand times more safe and innocent than spiritous liquors,” he wrote.)
Compounding the modern confusion about the nature of addiction, psychiatry keeps refining criteria for what it labels “substance use disorder.” In the current edition of its diagnostic manual, the D.S.M.-V, a person has a mild disorder if they meet at least two of 11 symptoms. The more the symptoms, the greater the severity of the disorder.
Research on drug use began to take off in the 1970s. By 1997 Alan I. Leshner, then the head of the National Institute on Drug Abuse, published the foundational position paper, “Addiction Is a Brain Disease, and It Matters.”
To the public, policymakers and even health care workers, he wrote, “Addiction as a chronic, relapsing disease of the brain is a totally new concept.”
But he did not overlook contributing factors. “Not only must the underlying brain disease be treated, but the behavioral and social cue components must also be addressed,” he wrote.
His much-cited research summary, which appeared a year after Purdue Pharma launched the highly addictive prescription opioid OxyContin, had a powerful, positive effect. The brain-disease designation would stimulate funding for research, be used to expand insurance coverage for treatment and prompt changes in public policy and criminal law, where newly minted drug courts—now increasingly called “recovery courts”—urged defendants into treatment. The brain-disease framework would eventually be adopted by mainstream medicine, including the surgeon general.
And it offered patients and families a building block toward compassion as well as ways to counter ubiquitous scorn.
The model continues to hold value, said Dr. Nora Volkow, who now leads the institute. She refers to addiction as “a chronic, treatable medical condition.”
In a statement, she added, “Acknowledging that addiction involves changes to the brain does not discount the many genetic, social, environmental and other factors that also play an important role.”
Whether the brain will ever sufficiently recover after long abstinence, however, needs further studying, argued a 2022 review of the research, though the authors suggested that evidence is promising.
But as academics wrestle with how to frame addiction, patients and loved ones struggle painfully with the lack of certainty.
Nadia, whose father fatally overdosed on fentanyl in 2023, said that defining addiction as a disease lets users off the hook of responsibility.
“It’s difficult to hear people call addiction a disease, like cancer or progressive illnesses,” wrote Nadia, who lives in Minneapolis but asked that her last name be withheld to protect her family’s privacy. “My father chose drugs, time and time again. He missed all three of my graduations, my wedding and the birth of my child, as well as all the milestones of my sister. It’s hard to be told that he can’t control it. That we weren’t important enough for him to overcome it.”
Nadia was among the hundreds of readers who responded to questions from The New York Times about their families’ struggles with substance use. Many said that they agonized: They were furious with the person using drugs or alcohol. Yet many also felt guilty for bitterly resenting a parent, sibling, child or spouse who, they also accepted, was sick with a disease.
“People want to relieve themselves of the burden of the mixed emotions they feel towards their loved one, but that’s the burden inherent in the condition,” said Keith Humphreys, a psychologist and an addiction expert at Stanford University. That is in part why, he said, it’s easier for people to see addiction in absolutist terms — as a choice or a disease.
Overwhelmingly, family members described their burnout. “When a loved one is addicted to drugs it’s like they’ve been bitten by a vampire,” wrote Robin Pratt, whose sister used opioids for a dozen years. “They never stop plotting what they can take from you to support their habit. The same person who, before drugs, you would have trusted with your life, becomes someone you wouldn’t even trust with your purse.”
Almost 30 years ago, when Dr. Leshner argued for the brain-disease designation, he did so in part to break through what he called the long-simmering “imprecision and misconception” around addiction.
He then added: “In fact, if it were possible, it would be best to start all over with some new, more neutral term.”
Credit: The New York Times
Experts highlight the effects of intermittent fasting on the body
Team Metabolic Health
It is crucial for individuals considering intermittent fasting to consult with a healthcare professional, particularly if they have underlying health conditions, mentioned Dr Kumar
Intermittent fasting (IF) has gained popularity for its potential benefits, including weight loss and improved metabolic health. However, concerns about its impact on the liver, a vital organ responsible for detoxification, metabolism, and digestion, and the heart are often not discussed.
Stating that intermittent fasting is a Western concept, Dr Shiv Kumar Sarin, gastroenterologist, the Institute of Liver and Biliary Sciences, told ANI, “IF requires you to eat in a particular window and to fast for 14 or 16 hours. That’s not a great idea. In fact, it can increase your cardiac problem.”
Let’s understand more about liver health (Source: Getty Images/Thinkstock)
Dr M Sai Sudhakar, director, Cath Lab, chief interventional cardiologist, chief cardiac transplant physician, Gleneagles Hospitals, Lakdi Ka Pul, Hyderabad said intermittent fasting, while popular for its potential health benefits, can have damaging effects on the heart if not approached carefully. “Prolonged fasting periods can lead to electrolyte imbalances, particularly in potassium, magnesium, and sodium, which are crucial for maintaining proper heart function. These imbalances can result in arrhythmias, or irregular heartbeats, which can be life-threatening. Additionally, fasting can elevate cortisol levels, the body’s primary stress hormone. Chronic high levels of cortisol increase blood pressure and heart rate, placing extra strain on the cardiovascular system and heightening the risk of heart disease over time,” said Dr Sudhakar.
However, Dr Ranjan Modi, senior consultant and head, interventional cardiology, Sarvodaya Hospital, Sector-8, Faridabad said research results on intermittent fasting are mixed. “Short-term studies suggest there is greater weight loss with intermittent fasting than with regular calorie cutting. But longer studies — from six months to one year — have not all found this to be true,” Dr Modi added.

Intermittent fasting and liver health: All you need to know (Source: Getty Images/Thinkstock)
A study from the American Heart Association’s Epidemiology and Prevention noted that restricting eating times to fewer than eight hours a day may be linked to a higher risk of dying of heart disease. “But a review of studies on intermittent fasting found that the weight and blood sugar changes reported were small. More research is needed to see whether regular fasting can reduce the risk of heart disease,” said Dr Modi.
Further, Dr Rajiv Kovil, head of diabetology, Zandra Healthcare and co-founder of Rang De Neela initiative said the liver is responsible for vital functions like aiding digestion, metabolism, detoxification, regulating hormones, and storing essential nutrients. “Non-alcoholic fatty liver disease (NAFLD) or fatty liver (steatosis) occurs when the fat starts to accumulate around your liver cells by slowing the process of breaking down fat,” said Dr Kovil.
From a medical perspective, Dr Chandan Kumar K N, senior consultant hematologist and lead T, Gleneagles Hospitals, Lakdi Ka Pul, Hyderabad said intermittent fasting generally does not damage different body parts like the heart or liver in healthy individuals. “In fact, some studies suggest that IF may have protective effects on the liver by reducing fat accumulation, lowering inflammation, and improving insulin sensitivity,” said Dr Kumar, adding that it can be particularly beneficial in preventing or managing conditions like NAFLD.
But according to a 2023 review published in Diabetes, Metabolic Syndrome and Obesity, although some studies suggest that IF may have potential benefits for NAFLD, the evidence is still “limited and inconclusive”.
However, IF could potentially stress the liver in individuals with pre-existing liver conditions, such as cirrhosis or advanced NAFLD, said Dr Kumar. “Prolonged fasting periods might lead to a drop in blood sugar levels, forcing the liver to work harder to produce glucose, which could exacerbate existing liver issues,” said Dr Kumar.
It is crucial for individuals considering intermittent fasting to consult with a healthcare professional, particularly if they have underlying health conditions, mentioned Dr Kumar. Personalised medical advice ensures that fasting practices are safe and appropriate for one’s health status, said Dr Kumar.
Credit: The Indian Express
Study reveals your nose can tell a lot about these hidden diseases
Team Metabolic Health
From acne to wolf’s nose, here’s how the nose can tell us a lot about our health.
The nose is a prominent feature on the face, but thanks to unconscious selective attention, we can choose to not let it get in our line of vision. However, even though the brain works hard to ignore this prominent feature from hindering our view, we should not take the nose lightly, for it can be the messenger of many hidden diseases. A recent study, led by Dan Baumgardt, University of Bristol, stated that the nose can help us diagnose external skin conditions and internal diseases.

The study states that the nose can help us diagnose external skin conditions and internal diseases. (Unsplash)
Acne vulgaris and acne rosacea:
Acne vulgaris is one of the most common types of acne that can affect the nose. It happens when the tiny glands in the skin get clogged and lead to blackheads. These blackheads can develop in larger lumps, get infected, inflamed and pus-filled and can scar the skin.
Acne rosacea, on the other hand, is an inflammatory skin condition that leads to reddening of the skin, mostly the nose and the cheeks. Acne rosacea can lead to rhinophyma – the condition where the skin of the nose starts to grow and thicken, making significant changes in the appearance.
Wolf’s nose:
Also known as Sarcoidosis, wolf’s nose is an inflammatory disease that can affect any tissues in the body, including the lungs and the lymph nodes. This condition can lead to bluish or purplish patches on the body, usually on the nose, ears, the fingers and toes. Sarcoidosis on the nose is referred to as lupus pernio.
Trigeminal trophic syndrome:
The damage to the trigeminal nerve can lead to this condition. The nerve branches in the area of the skin surrounding the nostrils can get damaged, leading to dysregulated sensation. This is categorised by numbness, desensitisation, or prickles. Repeated damage can also lead to ulcers around the nostrils. However, this is different from skin picking disorder, where a person may feel psychologically compelled to pick skin.
Disclaimer: This article is for informational purposes only and not a substitute for professional medical advice. Always seek the advice of your doctor with any questions about a medical condition.
Credit: Hindustan Times
Should women stop smoking before conception? Is there ‘no safe period’ for smoking during pregnancy? Study answers
Team Metabolic Health
A new study sheds light on whether women should stop smoking before conception and if there is ‘no safe period’ for smoking during pregnancy.
Most women stop smoking when they learn that they are with a child. Every cigarette packet comes with a warning against smoking while pregnant. But is there any ‘safe period’ for smoking during pregnancy? Should one stop before conception? A new study is answering all these questions.

Women should stop smoking before pregnancy, a new study suggests. (Pexels)
Break the habit of smoking while you’re trying to conceive
A new study from China published by the Journal of Epidemiology & Community Health found out that before pregnancy, even light smoking (one to two cigarettes daily) can lead to some ‘serious health issues’ for the newborn baby. The study also reaffirmed the common belief that smoking at any point during pregnancy is dangerous for the growing fetus. Therefore, it is better for women to break the habit while still trying to conceive.
The study collected data from birth certificates in the US National Vital Statistics System between 2016 and 2019. The researchers analysed 12,150,535 mother-newborns and the number of cigarettes smoked per day, ranging from 0 to over 20. They found that the timing of smoking cigarettes during pregnancy matters. Their research found that smoking should be avoided during all stages of pregnancy and debunked the myth that light smoking is not as harmful if you do it before you get pregnant in the first three months of pregnancy.
Health effects of smoking
There are several researches out there that document the health effects of smoking during pregnancy. They reveal that it can lead to a greater risk for premature birth, low birth weight, and developmental issues in the womb. Since the effects after birth are less understood, it has led many women to think it’s safe to smoke before and after pregnancy.
The research stated, “There is no safe period and no safe level of cigarette smoking shortly before or during pregnancy.” They added that the findings of the study ‘re-emphasise the need to prevent smoking initiation for non-smokers and to promote smoking cessation for smokers’.
Top of Form
What did the study find out?
The study found that “newborns of smokers showed a higher rate of requiring assisted ventilation after birth, assisted ventilation for over 6 hours, NICU admission for mechanical ventilation, and surfactant replacement therapy. They also showed more significant risks for sepsis, seizures, or issues with the brain.”
Additionally, “smoking before pregnancy was associated with a 27 per cent higher risk of newborn health issues. The risk was 31 per cent to 32 per cent if the mother smoked anytime during pregnancy.” The study added, “Even smoking 1 to 2 cigarettes a day before pregnancy led to a 16 per cent higher chance of newborn health problems. The risk rose to 31 per cent if they smoked 20 or more cigarettes a day.”
Credit: Hindustan Times
Eye Drops To Eliminate Need For Reading Glasses to Hit The Indian Market by October
Team Metabolic Health
Mumbai-headquartered Entod Pharmaceuticals launched “PresVu” eye drops made using pilocarpine – the medicine that treats ‘presbyopia’ by reducing the size of the pupils which helps to see objects up close.
Starting first week of October, prescription-based drops will be available across pharmacies costing Rs 350. The medicine is indicated for the treatment of mild to intermediate presbyopia for people aged 40 to 55 years.
After deliberating over the medicine for over two years, the drug regulatory agency has approved India’s first eye drops to remove the need for reading glasses.
On Tuesday, Mumbai-headquartered Entod Pharmaceuticals launched “PresVu” eye drops made using pilocarpine – the medicine that treats ‘presbyopia’ by reducing the size of the pupils which helps to see objects up close. Presbyopia condition is the age-linked decline in the eyes’ ability to focus on nearby objects and this condition typically becomes noticeable mid-40s and worsens until about age of late 60s.
In an interview with News18, Nikkhil K Masurkar, chief executive officer (CEO) of Entod Pharmaceuticals said a single drop of the medicine starts working in just 15 minutes and its effects remain for the next six hours. If the second drop is also poured within three to six hours of the first drop, the effect will stay even longer.
“Till now, there was no medicine-based solution for blurry, near-vision except wearing reading glasses, contact lenses or a few surgical interventions.”

Entod Pharmaceuticals specialises in ophthalmic, ENT and dermatology medicines and exports to more than 60 countries.
Who can buy this medicine?
Starting from the first week of October, prescription-based drops will be available across pharmacies costing Rs 350. The medicine is indicated for the treatment of mild to intermediate presbyopia for people aged 40 to 55 years.
Masurkar claims that the medicine is the first of its kind in India which is tested on Indian eyes and customised as per the genetic fulcrum of the Indian population.
“Similar medicines are available in foreign countries. However, those formulations are not tested on Indian eyes which are much different from caucasian eyes. We have made several changes in the formulation,” Masurkar said.
The product will be sold only on prescriptions by registered medical practitioners. The company has started training its field force to inform and educate doctors about the usage of the latest product.
Phase III successful, gearing up for post-launch surveillance
Masurkar explained that the company had applied for the DCGI approval in early 2022 and the company was asked to conduct phase III clinical trials.
“We conducted the trials at ten sites across India with more than 250 patients. The results and data were submitted to the regulatory agency. The subject expert committee approved the study and recommended for approval from the drug controller general,” he said.
82 per cent of the total 274 subjects did not face any side effects. Remaining patients reported minor transient side effects including irritation and redness in eyes, blurring of vision and headache. “These all were transient side effects and resolved in couple of days. Once patient adapts, there should not be issues. No patient was discontinued from the trial,” he said.
While the results of the study are yet to be published in a peer-reviewed journal, the company plans to conduct post-marketing surveillance at several big eye-care centres across India including All India Institute of Medical Sciences (AIIMS), New Delhi.
“We will get the results published in medical journals as well but right now, we are preparing for post-marketing surveillance which can help us understand the different aspects of the medicine,” Masurkar added.
Credit: news18.com
Novo Nordisk’s Ozempic shortage expected to continue into Q4
Team Metabolic Health
A box of Ozempic made by Novo Nordisk is seen at a pharmacy in London, Britain March 8, 2024. REUTERS/Hollie Adams/File Photo
Novo Nordisk (NOVOb.CO), opens new tab said the shortage of lower strengths of its diabetes drug Ozempic has deteriorated, with intermittent shortages for all strengths expected into the final quarter of 2024 due to increased demand and along with capacity constraints at some of its manufacturing sites.
In a note published by the European Medicines Agency (EMA) on Monday, the obesity drug maker recommended healthcare workers continue limiting treatment initiation of new patients on Ozempic and its other diabetic drug, Victoza, until the supply situation improves.
Credit: Reuters
Dialysis May Prolong Life for Older Patients. But Not by Much
Team Metabolic Health
In one recent study, the challenging regimen added 77 days of life after three years. Often, kidney disease can be managed in other ways.
Even before Georgia Outlaw met her new nephrologist, she had made her decision: Although her kidneys were failing, she didn’t want to begin dialysis.
Ms. Outlaw, 77, a retired social worker and pastor in Williamston, N.C., knew many relatives and friends with advanced kidney disease. She watched them travel to dialysis centers three times a week, month after month, to spend hours having waste and excess fluids flushed from their blood.
“They’d come home weak and tired and go to bed,” she said. “It’s a day until they feel back to normal, and then it’s time to go back to dialysis again. I didn’t want that regimen.”
She told her doctors, “I’m not going to spend my days bound to some procedure that’s not going to extend my life or help me in any way.”
Ms. Outlaw was mistaken on one point — dialysis can prolong the lives of patients with kidney failure. But a new study published in the journal Annals of Internal Medicine analyzed data from a simulated trial involving records from more than 20,000 older patients (average age: about 78) in the Veterans Health Administration system. It found that their survival gains were “modest.”

An at-home dialysis machine. Credit: Veasey Conway for The New York Times
Administration system. It found that their survival gains were “modest.”
How modest? Over three years, older patients with kidney failure who started dialysis right away lived for an average of 770 days — just 77 days longer than those who never started it.
“I think people would find that surprising,” said Dr. Manjula Tamura, a nephrologist and researcher at Stanford and a senior author of the study. “They would have expected a greater difference.”
Moreover, those patients spent less time at home; they were in a hospital, a nursing home or a rehab center for about 15 more days than those who never started dialysis.
Another group didn’t begin dialysis early but continued with “medical management” (which could help alleviate symptoms if needed), though half of them started dialysis at some later point. They lived for about the same amount of time as those who started dialysis right away.
“Our field has really been debating about the role of dialysis in patients who develop kidney disease in old age,” Dr. Tamura said. “It’s lifelong therapy and a major change to your lifestyle. It can lengthen life, but there are trade-offs.”
About a third of the population over age 65 have chronic kidney disease, according to the U.S. Renal Data System. The pluses and minuses of treatment add up differently for them than for younger patients.
Among older adults who progress to kidney failure, most also have diabetes and many have heart failure, pulmonary disease or other serious chronic illnesses. They may not be candidates for transplants, the only cure for kidney failure, either because they’re too ill or frail for surgery, or because the wait for donated kidneys can be yearslong.
About 13 percent of the patients with kidney failure who register with the Renal Data System begin peritoneal dialysis at home — a more common treatment in other countries but one that, with Medicare incentives to providers, is gaining ground in the United States, too. It involves filtering blood through the abdominal lining.
But a great majority, almost 84 percent in 2021, still turn to dialysis centers, despite the challenges of transportation and the significant time commitment. Hemodialysis, the treatment offered in centers, requires a catheter, graft or fistula to allow access to a patient’s blood vessels, and it can cause side effects like infections, fatigue and itching. And, as the new study indicates, dialysis often means more time spent in health care centers, where most older adults don’t want to be.

A patient undergoes dialysis treatment at the Cape Coral Kidney Center in Cape Coral, Fla.Credit: Zack Wittman for The New York Times
The alternative to dialysis goes by various names — medical management, conservative kidney management, supportive kidney care. In this scenario, nephrologists monitor their patients’ health, educating them about behavioral approaches, prescribing anti-nausea drugs like Zofran and diuretics like Lasix to reduce fluid retention, and adjusting their doses as needed.
Ms. Outlaw, for example, takes a diuretic, two blood pressure drugs and a phosphate binder, along with iron and calcium. Five years after her kidney failure diagnosis, she’s feeling fine, though sometimes a little weak or tired, she said. She still preaches once a month at Manifestation Church of Holiness in the neighboring city of Greenville.
Not everyone in conservative management remains that active. “Some of my other patients are in wheelchairs,” said Dr. Rasheeda Hall, a geriatric nephrologist who provides conservative care for Ms. Outlaw and others at the Durham VA Health Care System.
“They’re more complicated — we have to pay a lot more attention,” she said. “But they sleep in their own beds. They’re not in the hospital a lot. They have a better quality of life.”
Some older kidney patients find that strategy preferable, even if death should come a couple of months earlier.
Often, however, “if you ask patients, ‘Were you presented with a choice?’ many of them will say no,” Dr. Tamura said.
Dialysis “is definitely still the default,” Dr. Hall said. When she meets with older patients, “I say, ‘You know, dialysis is not the only thing — there are medications we have in our arsenal that can help,’” she said. “And they say, ‘Oh.’”
That response appears commonplace. Researchers at the University of Washington developed a “decision aid” — a booklet explaining conservative kidney management and its pros and cons — and tried it out on patients 75 and older with advanced kidney disease and their families. The goal: to prompt discussion of conservative management with a health care provider.
In the groups that received the booklet, about a quarter of patients and their relatives had such conversations. But among those who didn’t get the booklet, only 3 percent of patients discussed conservative management with a provider, and none of their family members did.
“I was quite pleased” with the results, said Dr. Susan Wong, a nephrologist and lead author of the study. “It can be intimidating for patients to bring up alternatives when a provider is pushing or recommending or positioning dialysis as the only right thing to do.”
In her clinic, she said, about a third of patients go to dialysis centers, a third begin dialysis at home and a third opt for conservative management without dialysis.
Practices are shifting somewhat among kidney patients and their doctors. The most recent statistics from the Renal Data System, for instance, show that the use of peritoneal dialysis at home more than doubled from 2008 to 2021; the proportion of patients traveling to dialysis centers declined.
“Several things in the kidney world appear to be getting better,” said Dr. Kevin Abbott, program director in the division of kidney, urologic and hematologic diseases at the National Institute of Diabetes and Digestive and Kidney Diseases.
The proportion of older Americans with kidney disease has fallen, in part reflecting the wider use of more effective blood pressure drugs in recent decades, he said. The new diabetes drugs that help reduce weight and blood sugar also show promise for treating kidney disease.
But it still often falls to patients themselves and their families to question whether they want to start dialysis, to ask about other options like conservative kidney management, and to weigh their choices.
If they’re waiting for health care professionals to alert them to the alternatives, they may have to wait quite a while.
Ms. Outlaw’s decision owed much to her spiritual beliefs. “I’ve had a good life, and I am still enjoying it,” she said. But “if I pass away, I know where I’m going. My relationship with the Lord is good.”
Like any kidney patient, she can always change her mind about treatment. But she insisted that she would not. “The Lord is taking care of me,” she said. “Dialysis is not in my future at all.”
Credit: The New York Times
Beat the bloat: 5 easy dietitian-approved tips to keep you feeling light and free
Team Metabolic Health
Feeling bloated can be a real downer, but you don’t have to put up with it. We’ve rounded up five easy, dietitian-approved tips to help you beat the bloat.
Ever had that “why did I eat so much?” moment when your belly feels like it’s about to burst? Bloating can totally ruin your day, leaving you feeling heavy and sluggish. And you’re not alone—nearly one in seven Americans experience this every week, according to a 2023 study published in Clinical Gastroenterology and Hepatology. That uncomfortable, tight feeling often comes with your abdomen swelling up, making you feel even more miserable. But don’t worry, there’s a lot you can do to ease the bloat. Simple lifestyle changes, especially in your diet and exercise habits, can make a huge difference in getting you back to feeling your best.

Check out five tips to reduce bloating and improve digestion according to experts. (Pexels)
Dt. Shubha Dhyani Senior Clinical Dietician, Founder & CEO, Right Diet With Shubha shared with HT Lifestyle five simple dietary tips to help reduce bloating.
1. Eat Smaller, More Frequent Meals
Consuming large meals can overwhelm your digestive system and lead to bloating as your stomach struggles to process the large volume of food. Instead, try eating smaller portions more frequently throughout the day. This approach helps maintain a steady flow of digestive enzymes and reduces the likelihood of overloading your stomach, which can prevent excessive gas and bloating. Aim for about five to six smaller meals rather than three large ones.
2. Reduce High-Fiber Foods Gradually
Fibre is essential for digestion and overall health, but an abrupt increase can lead to bloating and gas. High-fiber foods such as beans, lentils, and whole grains are known to cause bloating because they ferment in the gut, producing gas. To minimize this effect, gradually increase your fibre intake to allow your digestive system to adapt. Additionally, soaking beans and cooking them thoroughly can help reduce their bloating potential.
3. Limit Salt and Processed Foods
Excess salt can cause your body to retain water, leading to bloating and swelling. Processed and packaged foods are often high in sodium, so it’s beneficial to limit their consumption. Instead, focus on fresh, whole foods and use herbs and spices to flavour your meals. Reducing sodium intake helps manage fluid balance and can reduce bloating associated with water retention.
4. Stay Hydrated and Avoid Carbonated Beverages
Drinking plenty of water is crucial for digestion and can help reduce bloating by flushing excess sodium and waste from your system. On the other hand, carbonated beverages like soda can introduce extra gas into your digestive tract, leading to bloating. Opt for still water or herbal teas instead. Staying well-hydrated also supports healthy digestion and reduces the risk of constipation, which can contribute to bloating.
5. Incorporate Probiotics into Your Diet
Probiotics are beneficial bacteria that help maintain a healthy balance of gut flora. An imbalance in gut bacteria can lead to bloating and discomfort. Including probiotic-rich foods, such as yoghurt, kefir, sauerkraut, or kimchi, in your diet can improve digestion and reduce bloating. These foods help promote a healthy gut microbiome, which supports more efficient digestion and can alleviate bloating caused by digestive disturbances.
Following these tips can effectively manage and reduce bloating, leading to greater comfort and overall digestive health.
Credit: Hindustan Times
7 tips for parents to reduce child’s screen time as it could be leading to obesity, poor grades
Team Metabolic Health
Too much screen time could be turning your child into a zombie. Check out these 7 practical tips for parents on how to stop it
Excessive screen time can impact the child’s physical and mental well-being by impacting their sleep, mood, concentration and academic performance. We must understand how excessive screen time can take a toll on the child’s overall well-being, so we got an expert on board to roll out some practical tips for parents to regulate the screen time of their child.

7 tips for parents to reduce child’s screen time as it could be leading to obesity, poor grades (Photo by Today’s Parent)
In an interview with HT Lifestyle, Dr Anish Pillai, Lead Consultant – Neonatology and Paediatrics at Motherhood Hospitals in Kharghar, Mumbai, shared, “In today’s digitalised world, everyone is relying on smart gadgets, compared to traditional alternatives. From cookbooks to YouTube recipes, outdoor games to video games, meeting friends to online chatting, society is rapidly changing. Right from a young age, children are exposed to mobile phones, television, or tablets, to keep them engaged while eating or playing.”
He added, “These electronic devices provide respite to parents who are often busy with office work or household chores. However, this can increase their dependence on these devices and make them habituated. Children are more likely to mimic what they see, which is why most of their behavioural pattern is interlinked with the type of content they see. Excessive screen time can negatively impact their physical and psychological health.”
The following are some negative effects of excessive screen time in children –
Reduced attention span: Prolonged exposure to electronic devices can negatively affect attention span. This can cause side effects like difficulty in focusing on one task for a longer period, constantly being restless and fidgety, and trouble paying attention in class or while doing homework. That is because the content online often contains fast-paced images or scenes and a lot of exciting stuff all at once, resulting in constant brain stimulation. This is why kids often find slow-paced activities like reading or writing that require patience and focus as boring.
Poor academic performance: Your kids might often struggle to complete a single task without someone’s help. The key to keeping your kid’s brain active and sharp is learning new things and using logical reasoning to solve problems. When your child is busy engaging in watching online videos and games, they are constantly missing out on fun and brain-stimulating activities like chitchatting with others, playing games, or reading.
Obesity: Glued to an electronic screen for a prolonged period can limit one’s mobility. Sitting in one place for longer hours without taking a break can lead to sudden weight gain. This screen time is often accompanied by unhealthy snacks and treats that can significantly increase their calorie intake. Excessive weight gain can increase the risk of diabetes, heart disease, and high cholesterol levels.
Reduced social skills: In this ever-evolving digitalized era, kids have potentially forgotten the concept of socializing. They are often seen binge-watching videos on tabs or phones while attending social gatherings or parties. It becomes quite challenging for them to interact with others, meet new people, and make friends resulting in isolation and loneliness in the real world.
Practical tips to reduce screen time
- Encourage children to play outdoors with their friends to develop their cognitive skills.
- Use screen time for educational purposes, research, puzzles, and games for collective experience.
- Be attentive to the content your kid is watching. Ensure that you choose age-appropriate videos or games that help in improving their critical thinking.
- The American Academy of Pediatrics (AAP) recommends no more than 1 hour of screen time per day for children aged 2 to 5 and similar limits for older children.
- Parents should make strict rules by keeping electronic screens out of their dinner time, bedroom, and family time to create a healthy space for interaction and family bonding.
- Plan family outings to amusement parks, museums, libraries, and theatres to keep children engaged and involved instead of being glued to their smartphones.
- Parents should demonstrate healthy screen habits by limiting their own screen time and engaging in non-screen activities.
Credit: Hindustan Times
Diabetes medications might prevent memory loss and dementia? Here’s what your parents should know
Team Metabolic Health
Could your diabetes medicine protect you from dementia? New study suggests yes. These are the common type 2 diabetes meds that might protect against memory loss
Certain types of medicines used to treat type 2 diabetes might help to prevent some cases of dementia, according to new research that builds on previous evidence suggesting these drugs might be useful in countering debilitating diseases associated with memory loss and cognition.
New hope: These diabetes medications might prevent memory loss and dementia (Photo by Shutterstock)
Scientists found there was a 35% reduced risk of dementia associated with a class of drugs that includes AstraZeneca Plc’s Forxiga and Boehringer Ingelheim GmbH’s Jardiance, which are called sodium glucose cotransporter 2 inhibitors. They were compared with so-called dipeptidyl peptidase-4 inhibitors, a category that includes Novartis’s Galvus and Johnson & Johnson’s Invokana.
The study, using data from South Korea’s national health insurance database, was published in the British Medical Journal. It found that alongside a potential reduced risk for dementia associated with SGLT2 inhibitors, there was also a 39% reduced risk for Alzheimer’s disease and a 52% reduction in the risk for vascular dementia.
Because the study was only observational, it cannot ascertain cause and effect between the drug and the impact on dementia risk. The scientists have called for clinical trials to now be carried out to test this theory.
Other studies have also shown that SGLT2 inhibitors appear to be associated with a reduced risk of dementia.
“The mechanism through which these effects take place are unknown but likely relate to either affecting inflammation in the brain, reducing the risk for cerebrovascular events or modulating glucose metabolism in the brain,” said Ivan Koychev, senior clinical researcher at Dementia Platform UK, which is based at the University of Oxford. Re-purposing existing drugs for new indications also “reduces greatly the risk of the drug failing through safety concerns,” said Koychev.
Credit: Bloomberg
Gen-Z wellness revolution: Secret behind why they are spending big on beauty and health
Team Metabolic Health
Gen-Z’s obsession with health and beauty: Know the secret to confidence and success of the ultimate wellness warriors
Gen-Z is a very special generation in so many ways and their outlook towards health, beauty, wellness and finance is way different from other generations. They have a certain independence and awareness about what matters to them.

Gen-Z wellness revolution: Secret behind why they are spending big on beauty and health (Photo by Metro Parent)
McKinsey’s latest Future of Wellness research shows that Gen-Z is more interested in wellness spending that’s focused on appearance and overall health. In an interview with HT Lifestyle, Dr Rashmi Shetty, Board Certified Cosmetic Dermatologist, Owner and Founder of RA Aesthetic and Dermatology Clinic in Mumbai, revealed that every aspect of Gen Z’s life is determined by a need to put their best foot forward – be it in areas of financial independence, relationships, career goals and of course, their appearance and health.
According to her, some of the key reasons for this pivot in the generation are –
1. Evolution of beauty standards:
The concept of beauty is very different in the Gen-Z context. They are very particular about how they look and how they present themselves at work, in social gatherings or at parties. With all the information available, they are a curious generation that’s eager to know what goes inside their products, the sustainable choices they have whether in the skincare they choose or the makeup they use.
2. Onset of social media:
Gen Z have been a part of the social media boom and have seen the growth of Instagram, TikTok and other platforms. They value authenticity, real reviews and advice from influencers. They actually interact with brands on social media to raise concerns or resolve their challenges. It’s not a generation that’s submissive or laid back. They are highly motivated and make choices that keep themselves before other things. The visual-heavy medium is helping them look their best with all the guidance they have in doctors, experts, bloggers sharing information.
3. Witnessing a pandemic:
Gen Z has witnessed a catastrophic pandemic in their formative years. This has actually shifted their focus and made them more conscious of health and wellness. Covid-19 shaped them in many ways. It made them define their priorities and enabled them to take care of themselves physically, emotionally and financially.
4. Having an urge to excel:
Gen-Z are exposed to thousands of success stories, be it celebs or startup founders. They have a vision for themselves and are extremely self-aware. Excelling at whatever they pursue is the goal to success and not merely doing something to earn a living. They value the importance of impact and the consequences of their actions. This encourages them to choose best and look best at all phases and stages of their lives.
5. Having financial freedom:
This generation knows how to make money and how to use it constructively. They are not dependent on their life choices or decisions. They research, ask questions and prioritise the way they are perceived by the world. They are open to beauty treatments, skincare routines and sustainable skincare trends that make them look better and feel better.
Gen-Zers are clear, decisive and financially independent. They are unapologetic in the way they want to look. If they want to do their lips or colour their hair blue, they get it done. Unlike the previous generations they are not worried about what others would say. They are very financially independent and have a lot of financial freedom at hand.
How they perceive life is a summation of their experiences and observations of the world. That has played an integral role in their lifestyle choices and decisions. Studies have also shown their inclination towards things that were never centrestage for the other generations.
Just like how mental health is slowly being accepted and adopted, vanity is not looked down upon. The Gen-Z are open to taking care of their looks and even recommending their dermatologists openly. They take a lot of pride in pampering themselves and don’t shy away from putting their most beautiful self forward.
Credit: Hindustan Times
Why Is the Loneliness Epidemic So Hard to Cure?
Team Metabolic Health
In the early months of 2020, as the Covid-19 pandemic settled over the country, a psychologist and Harvard lecturer named Richard Weissbourd approached his colleagues with a concept for a new kind of study. Loneliness, or the specter of it, seemed to Weissbourd to be everywhere — in the solitude of quarantine, in the darkened windows of the buildings on campus, in the Zoom squares that had come to serve as his primary conduit to his students. Two years earlier, he read a study from Cigna, the insurance provider, showing that 46 percent of Americans felt sometimes or always alone. In 2019, when Cigna replicated the study, the number of lonely respondents had grown to 52 percent. God knows what the data would say now, Weissbourd thought.
Credit: Illustration by Max Guther. Concept by Alex Merto.
“Initially, the idea was, OK, we’ve got a problem that’s not new but is obviously affecting lots of us, and that is now more visible than ever — it’s more present than ever,” Weissbourd told me. “What I really wanted was to get under the hood. Like, what does loneliness feel like to the lonely? What are the potential consequences? And what’s causing it?”
Finding answers to these types of questions is a notoriously difficult proposition. Loneliness is a compound or multidimensional emotion: It contains elements of sadness and anxiety, fear and heartache. The experience of it is inherently, intensely subjective, as any chronically lonely person can tell you. A clerk at a crowded grocery store can be wildly lonely, just as a wizened hermit living in a cave can weather solitude in perfect bliss. (If you want to infuriate an expert in loneliness, try confusing the word “isolation” with “loneliness.”) For convenience’ sake, most researchers still use the definition coined nearly three decades ago, in the early 1980s, by the social psychologists Daniel Perlman and Letitia Anne Peplau, who described loneliness as “a discrepancy between one’s desired and achieved levels of social relations.” Unfortunately, that definition is pretty subjective, too.
In order to understand the current crisis, Weissbourd, who serves as the faculty director of Making Caring Common — a Harvard Graduate School of Education project that collects and disseminates research on health and well-being — created a 66-question survey, which would be mailed to approximately 950 recipients around the United States. With the exception of a couple of straightforwardly phrased items — “In the past four weeks, how often have you felt lonely?” — a majority of the queries devised by Weissbourd and the project’s director of research and evaluation, Milena Batanova, approached the issue elliptically, from a variety of angles: “Do you feel like you reach out more to people than they reach out to you?” “Are there people in your life who ask you about your views on things that are important to you?” Or: “Has someone taken more than just a few minutes to ask how you are doing in a way that made you feel they genuinely cared?”
Several weeks later, the raw results were sent back to Weissbourd. “Frankly, I was knocked back,” he told me. “People were obviously really, really suffering,” and at a scale that dwarfed other findings on the topic. Thirty-six percent of the respondents reported feeling chronic loneliness in the previous month, with another 37 percent saying they experienced occasional or sporadic loneliness. As Weissbourd and Batanova had hoped, the answers to subsequent questions helped clarify why. Among the cohort identifying as lonely, 46 percent said they reached out to people more than people reached out to them. Nineteen percent said no one outside their family cared about them at all.
The struggle was particularly conspicuous in young respondents, ages 18 to 25, a sizable majority of whom reported acute feelings of loneliness in the previous month. Unsurprisingly, those subjects said, the pandemic had made them lonelier; in some cases, they had effectively withdrawn from a world that no longer had much meaning to them.
In February 2021, around the time Harvard announced its plans for the resumption of in-person classes, Making Caring Common published the results of the survey. “We have big holes in our social fabric,” Weissbourd said in a news release accompanying the paper, which he had titled “Loneliness in America.” Almost immediately, the emails and calls — from reporters, from other researchers and from lonely Americans who saw themselves reflected in the research — began pouring in. They did not stop arriving for several months. “My read was that the pandemic had exposed and turbocharged an existing problem,” Weissbourd told me. “Everything was being accelerated.” And it continued to accelerate, long after the world reopened: In March 2021, a quarter of adult respondents to a Gallup poll said they felt lonely for “a lot” of the day; that same month, the portion of young people dealing with the emotion on a regular basis was close to 40 percent. The Gallup numbers have since dropped somewhat, but not everyone has reaped the same benefits: The American Psychiatric Association says that 25 percent of U.S. residents are lonelier today than they were before the pandemic.
Last year, the U.S. surgeon general, Vivek Murthy, issued a 71-page advisory warning of an American “epidemic of loneliness and isolation,” with all the danger that classification implies. Murthy has estimated that a lack of social connection currently affects more Americans than, say, diabetes or obesity. Together with a concurrent decision by the World Health Organization to make loneliness a “global public health concern,” the surgeon general’s report has helped nudge the emotion into the same cultural position held by depression in the era of “Prozac Nation” and anxiety in the early aughts: a celebrity condition to be unpacked in an apparently endless cascade of front-page articles and self-help books (see: “A Practical Guide to Overcoming Loneliness” or “The Path Out of Loneliness”). There are now hundreds of podcast episodes devoted to loneliness, as well as a slew of start-ups like Belong Center, an anti-loneliness nonprofit.
Japan and Britain, where loneliness is as much a concern as it is in the United States, even appointed ministers of loneliness — government officials tasked with plumbing the depths of the crisis and ameliorating it, whether through public awareness campaigns (“Your hobbies and interests are important.”) or initiatives, like one in Britain, in which mail carriers were asked to check in with the elderly residents on their routes. Murthy, for his part, has suggested that entertainment companies might create more content that “reinforces the core values of connection.” Individuals, he adds, should consider “being a positive and constructive participant in political discourse and gatherings (e.g., town halls, school board meetings, local government hearings).”
What all these various efforts share, to one degree or another, is the idea that the solution to loneliness is only a phone call, or an email, or a text, or a friendly door knock away — that the key to closing the gap between perceived and realized levels of interpersonal relations, on a societal scale, is ultimately a matter of restoring a world that has slipped away from us. But at best, this sort of thinking reflects a misunderstanding of how we live now (and how we’ll live in the future). At worst, it serves as a distraction from the real issues. As research like Weissbourd and Batanova’s demonstrates, when we talk about loneliness, what we’re actually talking about are all the issues that swirl perilously underneath it: alienation and isolation, distrust and disconnection and above all, a sense that many of the institutions and traditions that once held us together are less available to us or no longer of interest. And to address those problems, you can’t just turn back the clock. You have to rethink the problem entirely — and the potential solutions too.

Credit: Illustration by Max Guther. Concept by Alex Merto.
Compared with other ailments of the mind, loneliness is a surprisingly modern concern: Although large segments of the world have probably always been anxious, have always been depressed, have always been wrathful, they were not always lonely in the specific (and negatively connoted) way contemporary experts understand the emotion today. In her 2019 book, “A Biography of Loneliness,” the historian Fay Bound Alberti goes so far as to argue that before the 1800s, practically no one in the Western world spent much time discussing loneliness at all.
Which is not the same as saying that no one was familiar with the word: It gets dropped in Shakespeare’s “All’s Well That Ends Well”; in Samuel Johnson’s dictionary (“disposition to solitude”); and in “Robinson Crusoe,” a novel published in 1719. Still, as Bound Alberti writes, in most pre-19th-century literature, “there was no emotional experience necessarily attached to solitude.” If anything, it was often nice to be alone. It was as good as a spa day. You try living in a single-room farmhouse with 14 members of your family. You would crave some isolation, too.
In the appendix to “A Biography of Loneliness,” Bound Alberti includes a graph depicting incidences of the word “loneliness” in a database of English-language works printed between 1550 and 2000. From 1550 to 1800, the line hovers somewhere between zero and 0.0001 percent. Then comes the 1820s, and the line charges vertiginously upward, like a mountaineer ascending a cliff. No mystery there. The world was changing, fast. War, mechanization, the rise of the metropolis, war again. Communities disintegrated — sometimes as a result of conflict and sometimes because the residents believed they could find better opportunities elsewhere. People moved out of small towns and into vast, anonymous cities. As they did, they sought a new etymology to explain the emotional cost; when we look at Bound Alberti’s graph, that’s very likely what we’re seeing.
In the 1950s, a small cohort of American scientists began grappling, for the first time, with the causes and effects of this new modern malady — in the process establishing what is today the growing field of loneliness studies. Among them was David Riesman, a sociologist who framed the emotion as being inextricably entangled with absence. Postwar America was prosperous, Riesman allowed, but prosperity had encouraged Americans to care about the wrong things. “Other-directedness,” he called it in his best-selling book, “The Lonely Crowd,” which he wrote with Nathan Glazer and Reuel Denney. Today we would call it FOMO: Americans were constantly peering over their neighbors’ fences, admiring the barbecue kit, the pool. When they failed to get those things for themselves, loneliness set in.
Others were inclined to see the emotion as something significantly scarier — a genuine medical syndrome, potentially widespread, on the level of depression or mania. “I am not talking here about the temporary aloneness of, for instance, a person who has to stay in bed with a cold on a pleasant Sunday afternoon while the rest of the family are enjoying the outdoors,” Frieda Fromm-Reichmann, a German-born psychiatrist, wrote in a groundbreaking paper called “Loneliness,” which was published posthumously in 1959. Nor was Fromm-Reichmann referring to wistful artistic solitude or the raw emotions that arise after the loss of a spouse. Her interest was in truly debilitating loneliness, of the type she observed in growing rates in her patients — loneliness that was “nonconstructive if not disintegrative” and that led to “the development of psychotic states. It renders people who suffer it emotionally paralyzed and helpless.”
But how? And why? What ultimately moved our understanding forward was the application of biological science. “Echocardiograms, brain-imaging technology, blood and urine tests. Using those, you could actually measure what was going on inside the body of a lonely person,” the psychologist Louise Hawkley told me recently. You could move past the anecdotal to the provable.
Hawkley has been researching loneliness for nearly 30 years — along with her mentor and friend, the late psychologist John Cacioppo, she has overseen or worked on nearly a hundred publications that illustrate, in often graphic detail, the physiological toll loneliness takes on the lonely. It is thanks to Cacioppo and Hawkley, for example, that we know loneliness raises our blood pressure, negatively alters our cognitive functions, is associated with Type 2 diabetes and shortens our life spans. (Subsequent studies have linked the emotion to suicidality, Alzheimer’s and leukemia.) When Vivek Murthy, in his 2023 advisory, writes that loneliness “is associated with a greater risk of cardiovascular disease, dementia, stroke, depression, anxiety,” he is largely referencing work done by Cacioppo and Hawkley.
In one of their most innovative experiments, designed to show that loneliness can cause poor health instead of merely correlating with it, they hired a hypnotist to coax a handful of test subjects into a state of heightened loneliness. Once it was induced, the subjects’ blood pressure and inflammation levels surged. “We could essentially manipulate the physiological condition by changing how lonely they felt,” Hawkley says. “And those same people, when they were made to feel not lonely” — when the hypnosis was reversed — “everything bounced back.”
In the mid-2000s, Hawkley and Cacioppo funneled their combined research to date into a framework that Hawkley described to me as a “sort of grand evolutionary theory of loneliness.”
The results, released nearly two decades ago in The Journal of Research in Personality, manage to get at the roots of our present-day predicament as incisively as anything I’ve encountered. In essence, Hawkley and Cacioppo argue, early Homo sapiens, outgunned by all manner of long-toothed beasts and without natural armor, achieved safety through community — they learned “to employ and detect deceit, and to communicate, work together and form alliances,” as the authors have it. Or the successful ones did, anyway. (The rest were eaten.) Gradually, our brains evolved to prioritize togetherness, and conversely, to generate an anxiety response when we failed to find it.
Imagine the warm sensation you feel on walking into a room full of friends. Now imagine being excluded by the same friends by a game of catch — an example from a study cited by Hawkley and Cacioppo. According to them, brain scans of the excluded participants demonstrated “neural activation localized in a dorsal portion of the anterior cingulate cortex that is implicated in the affective component of the pain response.” A mouthful, but you get the gist: To Hawkley and Cacioppo, the subjects’ pain was evidence that loneliness was a biological signal, not dissimilar to a rumbling stomach. “What hunger does for food, loneliness does for social relationships,” Hawkley told me. “It’s supposed to motivate us and tell us we need more people around us or that we need support. It tells us that something is wrong.”
In worst-case scenarios, loneliness becomes a self-fulfilling prophecy — a snare that tightens with each effort to shrug it off. What you sometimes see is the onset of a kind of feedback loop, Hawkley told me: A person desperately wants not to be lonely, but fear and anxiety have convinced them their loneliness reflects a fundamental undesirability. “They are absolutely certain that they’re not worth talking to, that no one likes them, that they’re not a good person and that it’s all their fault,” Hawkley says. “The brain is being hijacked.”
In 2021, Daniel Maitland, a psychologist and associate professor at the University of Missouri-Kansas City, devised an EKG-based pilot study in which he assembled a group of self-identified lonely people and asked them to participate in a series of relationship-building exercises. The moment the test subjects were asked to disclose something personal to their peers, the readings on the monitors strapped to their chests escalated, indicating that vulnerability was a major stressor on their nervous systems.
There are two ways to parse these results. The first is that Maitland’s subjects were lonely precisely because intimacy was naturally fraught for them. The second is that they were trapped in their own heads, in thrall to Hawkley’s feedback loop. For these subjects, advice about attending a local town hall or church basement bingo, however well meaning, would be likely to fall flat, partly because of the fear impulse it would engender. But partly, too, because that variety of community gathering feels so antique and unappealing to many of us — the relic of a bygone era.
In 2000, Robert Putnam, the Harvard political scientist, published “Bowling Alone,” a book that famously documented a steady erosion in membership of organizations and groups that once bound so many Americans together — granges and churches, unions and library reading circles, athletic clubs and neighborhood improvement associations. Nearly a quarter-century on, the trend lines identified by Putnam have not been reversed. If anything, they’ve grown more pronounced, as have the related data on household status and family: In 2024, American marriage rates are far lower than they were at the midcentury mark, while the number of one-person households in the country has more than tripled to 29 percent.
Needless to say, marriage doesn’t negate loneliness — plenty of bad or abusive marriages are chillingly sad for the people locked inside them — and a single-person home is not synonymous with a lonely one. Still, it’s impossible to look at the aggregate data from the 1950s onward, including a new survey by Gallup on weekly attendance of religious services, which sank last year to 21 percent of the U.S. population, and not feel that something has been lost.
“I’m not suggesting that we should become more religious, but I want to just suggest to you that religious communities are a place where adults engage kids, stand for moral values, engage kids in big moral questions, where there’s a fusion of a moral life and a spiritual life,” Weissbourd said at a talk held in March at the Harvard Kennedy School of Government.
“A sense that you have obligations to your ancestors and to your descendants, where there is a structure for dealing with grief and loss,” he went on, repeating his opening caveat. “I feel urgently like we have to figure out how to reproduce those aspects of religion in secular life.”
Earlier this year, Weissbourd and Batanova conducted a follow-up to their 2021 loneliness survey, adding an open-ended prompt in which lonely respondents could try to account for the presence of the emotion in their lives. Many subjects cited a lack of “meaningful connection” as the primary culprit. This was true whether or not human companionship was available to them. Physical proximity wasn’t always the issue. Emotional proximity usually was. Consider the young mother who frets that her existence has been reduced to caring for her baby, or the respondent who complains that his or her “partner is only interested in the phone.” A third subject admits to having plenty of family around but to being undervalued by them. “Am surrounded,” a fourth writes, by people “who only are present in my life because am useful.”
Work — the office — appears to be of little help. Fewer Americans are finding purpose and meaning in their careers, and the ones who do are laboring in a drastically altered landscape. Post-pandemic, office buildings in every major city remain empty; something like 22 million Americans now work from home, communicating with their colleagues through Zoom or Slack. Whether or not you believe that “virtual commuting” is good for productivity, it is demonstrably bad for community building. A July report by Jeffrey Hall, a professor of communication studies at the University of Kansas, and a team of researchers asked 4,300 Americans to talk about their social circle; most respondents said they had met their close friends through school or work. But the numbers were skewed by age: People 51 years or older were more than twice as likely to have met at least one close friend at work as people under 30. “Removing the social aspect of work further encourages remote workers to keep their jobs at arm’s length,” Hall wrote in The Wall Street Journal. “This detachment could have the twin effects of maintaining a better work-life balance but leave workers lonelier than they would be had they made office friends.”
The residue of the pandemic, for all of us, has proved difficult to scrub away. Studies have shown that we emerged from quarantine with less ability to make eye contact or conduct ordinary conversation with acquaintances. “The interactions that make us less lonely come naturally to us, but they still need to be practiced, or our skills atrophy,” Ian Marcus Corbin, a Harvard Medical School philosopher and senior fellow at Capita, which helped fund Weissbourd’s study, told me. “And in 2020 and 2021, a lot of people who were in a formative period of their lives saw those muscles atrophy.” Concurrently, the usage of “frictionless forms of interaction,” like self-checkout displays or meal-delivery apps, ballooned. Corbin sees these developments as evidence of “cocooning”: a retreat into a digital world that provides everything you need except the thing you need the most, which is the “meaningful connection” mourned by respondents to Weissbourd and Batanova’s survey.
When I spoke this year with Julianne Holt-Lunstad, a professor of psychology and neuroscience at Brigham Young University, she summed up the aggregate effects of these losses in a cascade of statistics she had apparently committed entirely to memory. “You look at the data from 2003 to 2020, and you see that time alone has gone up in America, while time spent with friends and family has gone way down. Time spent with others, companionship levels: It’s all down,” she said. “Then if you examine data from the national Crisis Text Line, which has information from 1.3 million texts, you see the No. 1 issue people are reporting has to do with relationships. One in three texts is related to relationship stress; one in five involves lack of human connection. In some cases, disconnection is happening due to feeling lonely. In some cases, a person is objectively isolated.” She added: “We may lack social support; we may have poor-quality relationships. It all signals that we’re not having our social needs met.”
Traditionally, the moments Americans have been most afflicted by loneliness have also been moments of major societal change: It is no accident that David Riesman wrote “The Lonely Crowd” in the age of TV dinners and white picket fences that separated one neighbor from the next. “There’s a cyclical nature to it,” says Eric Klinenberg, a sociologist at New York University and the author of “Going Solo: The Extraordinary Rise and Surprising Appeal of Living Alone.” “You look through the literature, and you can read anxiety about loneliness in the early 1900s, when everyone started listening to the radio. Or later, when we worried that cars would lead to us driving away from our families and neighborhoods in search of something new. You can read it in the ’60s and ’70s, with the sexual revolution and the rise in divorce rates. Throughout, loneliness is a ready-made discourse, right? It’s always there for us” — our go-to explanation for the recurring sensation that the culture is changing too fast and leaving us behind.
If the loneliness “epidemic” today feels uniquely profound, Klinenberg believes, it is only because the current dislocation is occurring at an unprecedented scale. “We’re the first people in the history of the earth to see the conditions of social life change in this way,” he says. “And they’ve changed dramatically.” Political dysfunction, global warming, a waterfall of mental health crises — and on top of it all, a transformation, in the internet, in the way we communicate.
The easiest way to respond to these dislocations, and to try to account for the loneliness they elicit, is to wish them away — to try to jam the genie back in the bottle. Weissbourd calls it a “palpable nostalgia for old modes of closeness,” and it’s everywhere in the responses to his and Batanova’s follow-up survey, from earlier this year, in which subjects were asked if Americans today are lonelier than they were in decades past and if so, why. “Previous generations,” one respondent writes, “weren’t as self-centered and helped each other more.” Another speaks of a time when individuals “lived in closer proximity” and “relied on family members to a greater extent.” “It took a community,” a third says, “to survive.”
This sentiment, too, colors many of the various proposed policy fixes, like Britain’s mail-carrier plan or the 2023 guidance from Murthy, who suggests near the end of his advisory that lonely individuals “reach out to a friend or family member” and that parents encourage their children to participate in structured, in-person activities “such as volunteering, sports, community activities and mentorship programs.” One implication is that shrinking the gap between realized and desired social relations, and thus conclusively ending the loneliness epidemic, will merely be a matter of recreating, in some sort of updated form, the types of community alive in an older era.
Unfortunately, history rarely works that way. “One big problem I have with the current rhetoric around loneliness is that we treat it as if it’s permanently going in only one direction,” Klinenberg told me. “It’s not. It’s a more interesting phenomenon than that” — and more nuanced. When loneliness gripped the Western world during the Industrial Revolution, everyone didn’t suddenly retreat to their ancestral villages; the radio didn’t make us permanently lonely. We built new communities in the city, far from our families; we used radio to expand our world and to talk to people on the other side of the country. We adapted. And as hard as it may be to accept, the path out of loneliness in 2024 lies almost certainly via a similar route — forward, forward.
There are signs that a similar mass evolution is already underway. Take the smartphone, a device that gets a lot of blame for our lack of physical connection and that has simultaneously led to other, but no less meaningful, forms of togetherness. “I wrote an entire book about online dating, and to give you one example, I know as much as anyone about how much it can suck to be on Tinder,” Klinenberg says. “I also know the internet is the main way people meet their spouses these days. I think about cases of people who have rare diseases and are able to share information and get better care and feel connected because the internet allows them to do so. I think about trans kids, who are at risk of distress because they feel so rejected and alone in some families and are now able to talk to people like them — to get messages that affirm them.”
None of which is to say we won’t still need physical togetherness — only that there may be less of it, and the physical togetherness that does persist may look different than it did for our ancestors. Ninety-six thousand Taylor Swift fans singing in sync, the thunder of a crowded football stadium and then a gazillion internet threads in which the attendees relive and post photos and remember the euphoria of their shared experience. A romance that exists partly in the real world and partly online, and in which emotional closeness is not diminished but enhanced by a steady stream of the sort of soul-baring disclosures that social media apps can facilitate.
There may be bumps, hurdles and obstacles, but as is the case with Cacioppo and Hawkley’s evolutionary theory, those bumps could be part of the learning process, the adaptation process. Part of the drive that forces us together.
Squint, and you can see it: a scenario in which the loneliness crisis today is really a mass period of acclimatization. It’s a bridge, an evolutionary step, during which we make our peace with certain trade-offs and realities — that in 2024, we’re not all going to race to rejoin the local grange. That we’re not all going back to church or temple or the mosque. That our kids may grow up far from their grandparents and aunts and uncles — far from the towns where we were raised. That the workplace will remain diffuse, tethered by Zoom meetings and the occasional in-person happy hour. That we may often see friends more on FaceTime than we do in real life. And most important, that despite it all, we’ll find one another again.
Credit: The New York Times Magazine
The Mosquito-Borne Virus Raising Alarms in the Northeast
Team Metabolic Health
Recent infections from the Eastern equine encephalitis virus are worrying health officials. Severe cases can be deadly or leave lasting injuries.
Residents of 10 communities in Massachusetts have been warned to stay indoors from dusk to dawn. Some local parks are closed at night. A person in New Hampshire has died. Pesticides are being sprayed from trucks and aircrafts.
What’s causing all of the alarm? A mosquito-borne virus called Eastern equine encephalitis, which is so rare that most infectious disease experts might never see a case. This year, at least four states have reported human E.E.E. infections.
Here’s what you should know:
Experts say that anyone who spends extended periods of time outside and around mosquitoes is at higher risk of contracting Eastern equine encephalitis. Credit: Jon Cherry/Getty Images
Is this an unusually bad year for E.E.E.?
The virus is endemic in North America, which means that it’s consistently present on the continent. The United States sees a handful of infections every year, mainly along the East Coast and around the Great Lakes. In 2019, there were a record 38 cases, the largest U.S. outbreak in recent history.
As of Tuesday, the Centers for Disease Control and Prevention had reported four human cases, in Wisconsin, New Jersey, Massachusetts and Vermont. In addition, officials in New Hampshire have reported one death.
But experts say it’s too soon to know whether this will turn out to be a particularly severe year. Mosquito-borne illnesses usually spread widely until around October, or when it’s cold enough for water to freeze, said Dr. Jonathan Abraham, a clinical infectious disease specialist at Harvard Medical School.
Until then, health officials in the affected areas are urging residents to take precautions.
Who should worry?
The main risk factor for contracting the virus is exposure to mosquitoes, said Dr. Cameron Wolfe, a professor of infectious diseases at the Duke University School of Medicine.
Those who spend extended periods of time outside — including people who have outdoor jobs, who are homeless or who enjoy hiking or biking — are at higher risk of contracting the virus simply because they are more likely to be bitten by mosquitoes.
They should consider taking extra precautions, like wearing long pants and shirts and using bug spray. Notably, not all outdoor areas are equally risky.
Walking around in downtown Manhattan is probably much less risky, Dr. Wolfe said, than spending time outside in a swampy, lowland area of South Carolina, for example — the sort of environment that mosquitoes love.
Where does the virus circulate?
In the life cycle of the E.E.E. virus, humans are sort of an afterthought. In swampy ecosystems, mosquitoes feed on infected birds and then pass the virus on to healthy birds.
Some species of mosquitoes feed on both birds and larger animals. These are the biters that infect people. Humans cannot transmit the virus to other humans, and mosquitoes don’t usually become infected after biting humans because people don’t have high viral concentrations in their blood. That’s why humans are considered “dead-end hosts.”
So, too, are the other animals that may fall ill with the infection, like ostriches, llamas and, as the name suggests, horses. The E.E.E. virus was first identified in the 1930s using cultures of infected horse brains.
What’s the illness like?
Most people who are infected with the E.E.E. virus have no symptoms or have flulike symptoms that resolve within a few weeks, according to the C.D.C. But if the virus reaches the brain — which happens in less than 5 percent of cases — the prognosis becomes dire.
Once in the brain, the virus attaches to proteins on the surface of neurons and kills them, often causing lasting neurological damage. The body’s immune response, which leads to swelling and inflammation, may also injure the brain, said Dr. Kevin Gobeske, a critical care neurologist at the Yale School of Medicine.
About 30 percent of patients who develop neurological symptoms die, according to the C.D.C. Survivors may be left with severe, long-term conditions like paralysis, intellectual impairment and personality disorders.
Is there a treatment?
There are no treatments that target the E.E.E. virus, so doctors focus on managing symptoms with pain medications or, in severe cases, using steroids to control swelling. “We don’t have many good options,” Dr. Gobeske said.
It’s not clear why some people recover fully while others are hospitalized with E.E.E. infections. There is not enough evidence to say whether particular groups are at higher risk of severe illness, Dr. Abraham said.
While there are vaccines for horses, none are approved for humans. The disease is rare and complicated enough that there hasn’t been a push to develop a vaccine for people, Dr. Gobeske said.
The best preventive strategy is to limit exposure to mosquitoes by dumping out standing water, repairing damage to door or window screens and, in some high-risk areas, avoiding outside activities after dusk.
Even if E.E.E. has not been reported in your state, Dr. Wolfe recommends taking these precautions to help avoid all mosquito-borne illnesses, like West Nile virus, that peak around this time of year. Several states have reported cases of illness from West Nile, with the most notable being Dr. Anthony Fauci, who has hospitalized with it this month.
“I don’t know a good, healthy reason you should be happy about being bit by a mosquito,” he said. “It doesn’t matter if it’s malaria, dengue or Eastern equine — there’s no particularly good outcome.”
Credit: The New York Times
Power Of Meal Timing: Expert Explains How Chrono-Nutrition Can Transform Your Health
Team Metabolic Health
Chrono-nutrition is understanding meal timing in alignment with the body’s internal clock. Read on to learn how it affects your health.
Have you ever noticed how certain meals leave you feeling energised while others make you sluggish? It turns out that when you eat might be just as important as what you eat. This concept, known as chrono-nutrition, is about aligning your meal times with your body’s natural rhythms to maximise health benefits. We spoke to our expert Dr Rohini Patil, MBBS and Nutritionist Founder, Nutracy Lifestyle, who explained chrono-nutrition and how it affects your health.
Chrono-nutrition is the process of understanding meal timing in alignment with the body’s internal clock, or what’s called acircadian rhythm. The body has different physiological cycles regulating metabolism, hormone secretions, sleep, and wakeups, said Dr Patil. According to a 2023 study, Among the various dietary strategies, chrono-nutritive therapy, which is grounded in chronobiology, emphasises consuming the majority of calories and carbohydrates during lunch and the early afternoon, while avoiding late evening meals.

The Science of Meal Timing
Metabolism and Insulin Sensitivity
“Recent studies have shown that the body processes food at different rates during different times of the day. Sensitivity to insulin, for instance, appears to be maximal during the morning hours and decreases as the day progresses,” said Dr Patil.
This may imply that the bulk of carbohydrates should be taken in the morning to achieve better blood sugar control and reduce the chances of getting diabetes. If we eat late into the night when insulin sensitivity is very low, glucose metabolism will be impaired, leading to weight gain.
Weight Management
“Quite a few studies have directly linked late-night eating to weight gain and consequently to obesity. Eating large meals or high-calorie food before bed may disrupt circadian rhythms and change your body’s way of handling food,” added Dr Patil. Chrono-nutrition says the bulk of your daily calories earlier in the day are more in sync with natural metabolic swings and might help in more effective weight management.
Digestive Health
The digestive system operates on a circadian rhythm, just like other body systems. Eating at irregular times can disrupt digestion and lead to issues like acid reflux or indigestion. By adhering to regular meal times that align with the body’s rhythm, you can support healthy digestion and reduce the likelihood of experiencing these problems.
Sleep Quality
Meal timings can affect sleep patterns. Heavy meals or late-night snacks may cause discomfort while sleeping or, perhaps affect digestion that may lead to poor sleep. Finishing one’s meals at least 2-3 hours before bedtime may help improve the quality of sleep and overall rest one gets.
Practical Chrono-Nutrition Tips To Follow
- Start with a Good Breakfast: Kick-start your day with a well-done breakfast containing proteins, healthy fats, and whole grains.
- Eat at Perfect Intervals: Try to consume a heavier diet during the part of the day. This way, in theory, it follows your natural body cycle and should keep your metabolic efficiency at its best for weight maintenance.
- Stick to the same regular eating times: Metabolic health is maintained when meals are taken at the same time from day to day.
- Avoid eating late at night: Shun food after dinner as much as possible. If one needs to eat something, then the food should be light, and something easily digested.
- Listen to Your Body: Listen to how different eating times affect your energy, mood, and well-being overall. Adjust mealtimes based on your body’s cues.
Bottomline
Dr Patil concluded, “Chrono-nutrition suggests that more than the quality of food itself, meal timing can be important for health. Syncing your meals with your body’s circadian rhythm may enhance metabolic efficiency, improve weight management, support digestive health, and get better sleep.”
[Disclaimer: This article contains information provided by an expert and is for informational purposes only. Hence, we advise you to consult your own professional if you are dealing with any health issues to avoid complications.]
Credit: onlymyhealth.com
Tips for international students to deal with unique mental health challenges and resources they should know about
Team Metabolic Health
It is crucial for international students to understand and access mental health support in order to thrive academically and personally.
Navigating the challenges of studying abroad can be both exhilarating and daunting for international students. In addition to the excitement of experiencing a new culture and academic environment, many face significant mental health challenges, which are often worsened by isolation, financial constraints, cultural differences, and the pressure to succeed. It is crucial for international students to understand and access mental health support in order to thrive academically and personally.

Studies have shown that international students often report higher levels of stress and psychological distress compared to their domestic counterparts.(Unsplash)
The Unique Challenges Faced by International Students
International students often encounter stressors that differ from those faced by domestic students. These include difficulties in adjusting to a new cultural environment, being independent, language barriers, and a lack of familiar support systems. Additionally, many students experience acculturation stress as they struggle to adapt to a new learning environment, interact with students from various nationalities, and reconcile their own cultural values with those of the host country. This can lead to feelings of loneliness, anxiety, and depression. Studies have shown that international students often report higher levels of stress and psychological distress compared to their domestic counterparts.
One significant barrier to seeking help is being self-aware of the impact of these changes, which is furthered by the cultural stigma surrounding mental health in many countries. In some cultures, openly discussing mental health issues is not common, which can prevent students from seeking support. Additionally, the fear that mental health services may not be culturally sensitive or relatable can further discourage them from seeking help. Understanding these challenges is the first step toward providing adequate mental health support to international students.
Resources Available for Mental Health Support
Many universities recognize the unique challenges faced by international students and have developed specialized resources to support their mental well-being. These resources typically include:
On-Campus Counseling Services: Most universities offer tailored counseling services for international students. These services often provide culturally sensitive counseling and therapy sessions, which can be crucial for students who may feel more comfortable discussing their issues within a familiar cultural context. Additionally, some universities offer drop-in sessions and online therapy options to make it easier for students to access support.
Peer Support Programs: Many institutions have peer support programs where international students can connect with others from similar cultural backgrounds. These programs help reduce feelings of isolation and provide a sense of community. Mentorship programs, where upper-year students guide newer students, are also common and can be a valuable resource for navigating both academic and personal challenges.
Workshops and Support Groups: Universities often host workshops and support groups focusing on mental health, stress management, and cultural adjustment. These sessions provide practical tools and strategies for coping with the challenges of studying abroad and offer a space for students to share their experiences and learn from others.
Community and Off-Campus Resources: In addition to on-campus services, students can access mental health resources within the wider community. Local mental health centers, hotlines, and online platforms offer various services, including counseling, therapy, and crisis intervention. Some services are specifically designed for international students, with counselors who understand their unique challenges.
Tips for Managing Mental Health as an International Student
While accessing formal support is essential, students can also adopt several self-care strategies to manage their mental health effectively:
Stay Connected: Maintaining relationships with friends and family back home is vital. Regular communication can provide emotional support and help reduce feelings of homesickness. Building a social network in the host country can also foster a sense of belonging and alleviate loneliness.
Practice Self-Care: Prioritize self-care activities that promote well-being. This includes getting enough sleep, eating a balanced diet, exercising regularly, and taking time for relaxation and hobbies. Simple practices like journaling, meditating, or spending time outdoors can significantly impact mental health.
Set Realistic Expectations: Students should set realistic academic and personal goals. The pressure to excel in a foreign environment can be overwhelming, so students should be kind to themselves and recognize that it’s okay to struggle sometimes. Seeking help when needed is a sign of strength, not weakness.
Engage in Campus Life: Participating in campus activities, clubs, and organizations can help students integrate into the university community and build meaningful connections. Cultural exchange programs can also enhance students’ understanding of the host culture and reduce cultural shock.
Seek Help Early: If students notice signs of mental distress, such as persistent sadness, anxiety, or difficulty concentrating, it’s essential to seek help early.
Wrapping it up
The mental health of international students is a critical issue that requires attention from both universities and students themselves. By understanding the challenges, accessing available resources, and adopting effective self-care strategies, international students can successfully navigate their academic journey and enjoy a fulfilling experience abroad. Universities, in turn, must continue to develop and promote services that cater to the diverse needs of their international student population, ensuring that they feel supported and valued throughout their studies.
(Author Patriek Karayil is President of American Colleges, the international arm of the American Education Board. Views expressed are personal.)
Credit: Hindustan Times